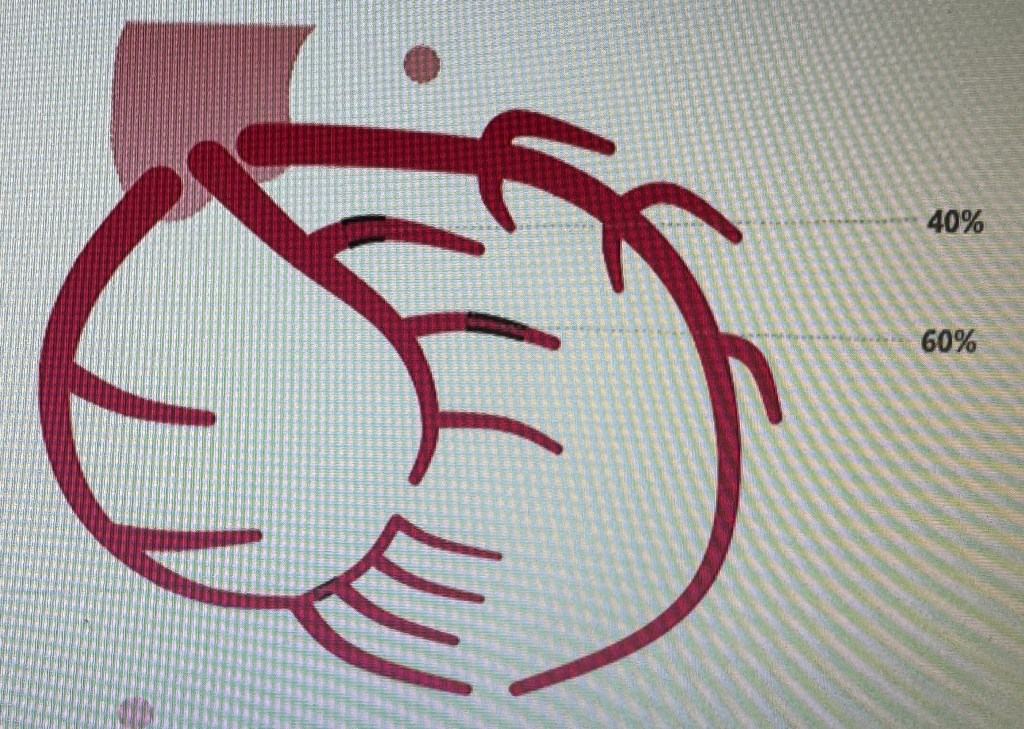
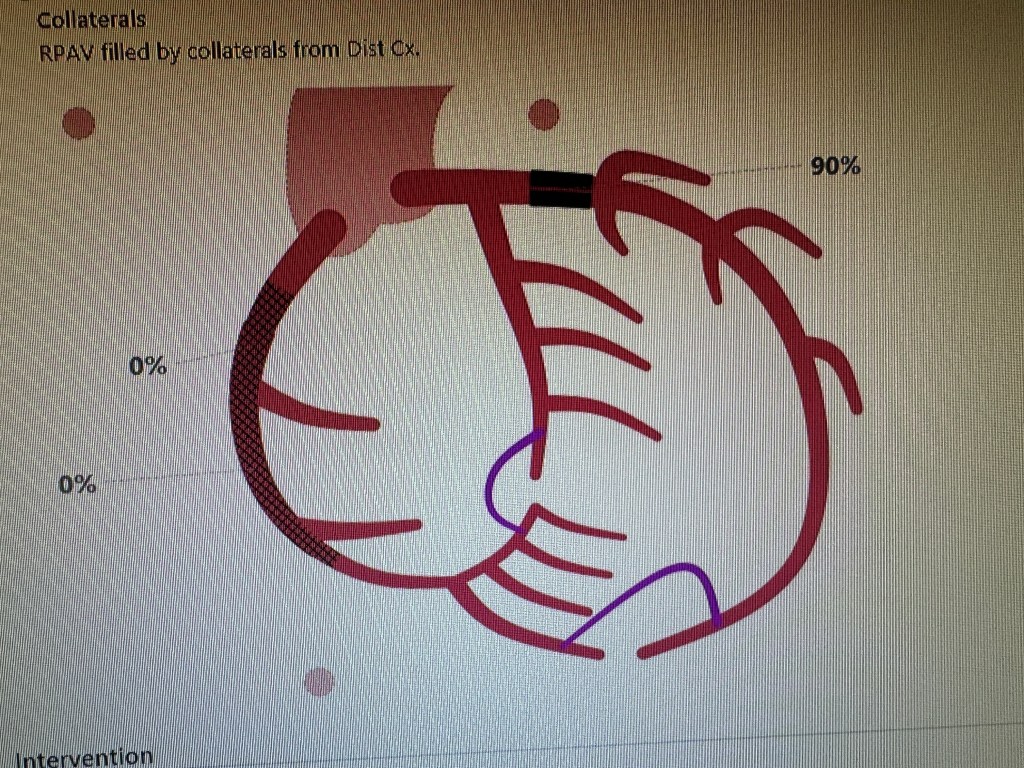
by Amin H. Karim MD Here is a case of the Left Circumflex coronary artery arising from the right sinus of Valsalva. (Type I anomaly). This happens in 0.3-0.6 percent of cases. Patient was a 42 year old lady presenting with atypical chest pain. The anomaly is usually benign but can be associated with non atherosclerotic coronary artery disease and myocardial infarction.
Left anterior descending coronary artery
Right coronary artery arising from its own ostium
The left circumflex arising from the right sinus of Valsalva separately ( Type I)
There is moderate occlusive disease in the branches of the left circumflex and the posterior descending coronary artery. It was decided to treat medically. The anomaly brought to memory the pre-stent days of plain balloon angioplasty. We had a similar case in the 1980s presenting with unstable angina. Cath showed the anomalous origin and an ulcerated plaque in the body of the circumflex. We proceeded to do balloon angioplasty. Unfortunately, the artery dissected. We knew as trainee fellows that this was bad news. There were many measures which interventional cardiologists took to “tack up” the intimal dissection and restore the flow to the artery. Most common first attempt was to advance the same balloon back and try longer inflations as much as the patient could tolerate watching the ST Segments and the blood pressure and listening to the patient. If that did not work we tried larger balloon with low pressure inflation. In some cases it would make the dissection worse but worked sometimes. Some attendings would would try to find where the dissection started proximally and start dilating there. In any case, the procedure would go on for long. Late Dr. John Lewis would get suggest that this was all “inflammation of the artery” and would give ibuprofen to the patient. When this would not work and the artery would look more messed up he would say that “there is more trouble in the artery than in the middle of downtown Beirut” keeping in mind there was war going on in the Middle East at the time. In the meantime, the irate cardiologist who was to follow in the same room would be watching from the glass partition. And the good cardiovascular surgeons who graciously gave us “surgical backup” (mandatory in those days) would be waiting in the wings to see when we got tired to let them take the patient to the OR and operate….. 🙂 Those were the days….. (Amin H. Karim November 30 2013)
This is continuing of the Journey in Private Practice starting from July 1987 and onwards. Marketing efforts for a specialist (non primary care) solo practitioner whose only source of patients is either patient referral, word of mouth, social media, or some other colleagues in primary care, is a ongoing process that has to go on as long as the practice has to continue. This is especially try in a competitive area. Here are some other ways which AngioCardiac Care of Texas employed to remain in focus.
WRITING IN LAY PRESS: This is not difficult to do. Any public health topic can be addressed to help other people understand diseases and procedures available and prevention measures to be taken. It’s a noble thing to do, in any case regardless.
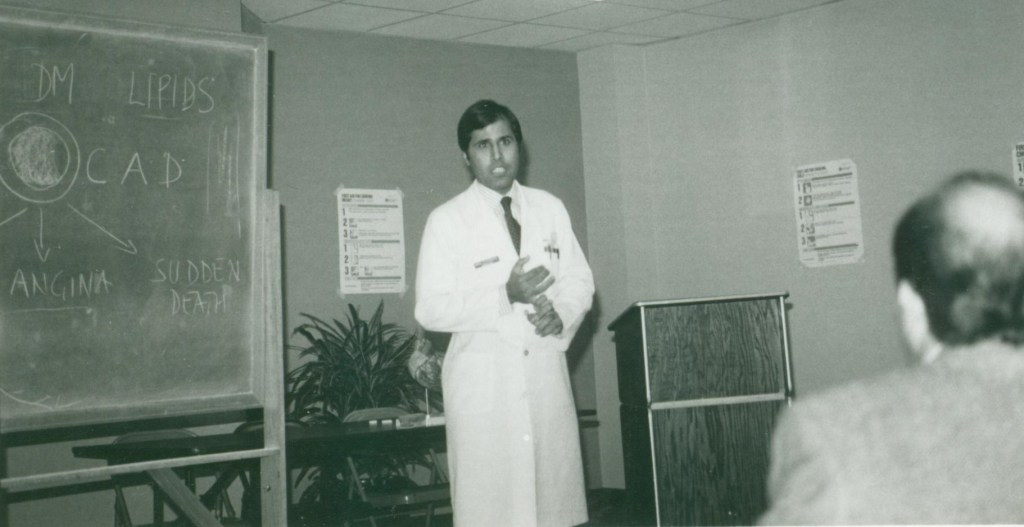
GIVING TALKS TO HOSPITAL MEDICAL STAFF: One gentle way of marketing effectively involved giving a Cardiology talk to hospital medical staff or primary care physicians, whenever an opportunity came forward. Topics would include Risk Factors, Screening for Heart Disease, New technology in Cardiology, topics that would interest them.
This section will recount in the journey some encounters with entities that representing venture (vulture) capitalists that come to town having done their homework which tells them that there are lot of dollars in the medical world. They also know most doctors are busy in their practices and have little time to look into other sources of income. So if they can be enticed into investing a little capital, sign up to work in the facility and get dividends they can have era income to supplement their practice income. Pretty simple concept and the share of limited partnership would conform to the Federal kick back laws. I recall some of these (all are in public domain). Some were very successful for all parties concerned and some not so successful, some never got off the ground an some utter failures were the physicians lost everything.
HIGHLY SUCCESSFUL! The one venture that has always impressed me and still does is the TEXAS ORTHOPEDIC HOSPITAL in Houston. in the early 90’s a large orthopedic group called the Fondren Orthopedic Group partnered with Hospital Corporation of America (HCA) to build a hospital dedicated to Orthopedic Surgery only with related entities like Radiology and Physical Therapy. There were about 20 partners in the group. I am not privy to what the financial arrangement was but word on the street was that the HCA would manage and operate the hospital in return for 20% of income and the rest would go to the Physician Partnership. The surgeons would use the hospital for most of their work. The model proved to be a great success. The hospital added a third floor and parking lot and continues to thrive with 50 plus orthopedic surgeon in one big group.
A second venture that proved very successful was the NORTH CYPRESS HOSPITAL on Highway 290 in Cypress. An entrepreneur made a mid size hospital with processional building and made physician own limited partnership interest in the hospital. The secret to their success was out of network billing which brought them huge profits and dividends to primary care and specialists who were partners and who worked at the hospital. For a while it worked till the savvy insurance carrier realized that patient with out of network benefits were preferentially being treated at the hospital. I think were lawsuits and not sure how they all ended. In any case the hospital was eventually sold to HCA System which now owns and operates the hospital.
A 85 year old dialysis patient who presented with non stemi last week; we stented his occluded RCA with good result and brought him back today for his LAD lesion; looked straightforward but the access to LM proved to be a challenge being on the roof of the sinus in a dilated aging aorta. The lesion itself looked juicy and inviting! 🙂 Iliac was tortuous so we ended up kinking a few catheters till we decided to beat it and go with the longest 7F sheath in the arsenal and a FR 3.5 came to our rescue. The rest was a piece of cake with predilatation and a Resolute Onyx Drug eluting stent 3.0 x 18 stent post dilated with 3.5 mm NC. According to Dr. Waqas Qureshi, MB guide would be another option in cases of wide aortic roots.
If one jumps into a solo practice, one of the first items on the agenda is how to market the practice. Back in 1980’s here is what I did. Things are bit different now but the samem principles apply:
Making friends with Primary Care Physicians: I made a list of as many primary care physicians in the area as I could find; target was independent physician offices and excluding those connected with the Medical Schools, VA System, County Hospitals etc since they were obligated to refer within the system. When time allowed I would visit each one of them and provided they were not busy with patients meet with them and leave business cards. Remember the 3 words that someone taught me a long time ago: be AVAILABLE, ACCESSIBLE AND AFABLE! Not all PCPs are easy to convince and break away from the usual referral patterns or ” buddy networks” but even a few breaks are welcome and once you start working with them and impress them with your communication and good care, you may get a long term referral source. More convincing is if the patient goes back and says good things about you.
Arranging an talk at a restaurant on a cardiology topic that would interest other physicians. This would take some investment or if one is lucky a drug rep might offer to underwrite the expenses. This is as long as they understand that your talk will be unbiased.
Buying an infomercial on local TV or radio. Luckily I was approached by a Spanish TV station to be interviewed by an anchor and answer questions on cardiac topics. Same with local radio stations. This gets your name out in the community.
Organizing special events: (1990s) Here we learned something from Prof. Denton Cooley. Although, Dr. Cooley was full resident of St. Luke’s Episcopal Hospital, and on faculty at the University of Texas, Houston and founder and Chair of the Texas Heart Institute, but in fact he was a private practitioner just like the rest of us independent cardiologists. He has about 6 partners in his practice and he had an exclusive arrangement with St. Luke’s such that no other CV surgeon could have privilege to do surgeries at the hospital unless they joined his practice. It was rumored that even Dr. Michael Reardon, who was his fellow, got independent surgery privileges at St. Luke’s. As a result, Dr. Reardon ended up going to next door Methodist Hospital ( a big gain for Methodist as Dr. Reardon established a very good practice and continues to be a busy CV surgeon at Methodist. In any case, Dr. Cooley excelled in marketing his practice. A cardiologist Dr. Virendra Mathur, was his referral and with him Dr. Cooley would visit Bombay, India and meet cardiologists there, ensuring a steady referral from India. As expected, these referrals would be well to do people or VIPs paying cash to St. Luke’s. (which had a good cash pay program for overseas patients). Personalities like Bollywood singer and actor Kishore Kumar and Pakistani nightingale singer late NoorJejan came to St. Luke’s for their CV surgery. So di many industrialists from Pakistan, some of who later became my patients once they found that there was a Pakistani descent cardiologist just next door to St. Luke’s. Locally, Dr. Cooley would organize a get together of his referral cardiologists every holiday season at his beautiful ranch in Rosenberg, Texas called the Cool Acres Ranch. It had streams running through it and 5 big houses. He would arrange a barbeque and fire works for children. We would have a good picnic at his ranch. It was friendship, camaraderie, marketing and goodwill all rolled into one and showed his talents, outside the operating room. He was a pleasant and friendly person who treated his colleagues with respect. His surgical skills do not need any praise as he was outstanding. In later years, he would not keep up with the advances in CV surgery like mini-cab with smaller incisions and off pump CABG, calling them ” mere gimmicks” ( as he once told me). But his legend, like that of Dr. DeBakey lives on at the Texas Heart Institute Building.
TAKING PART IN HEALTH FAIRS: One way to spread the word about your practice was to take part in Health Fairs, some organized by the hospital system, some by the local community associations (eg Association of Pakistani-Descent Physicians of North America APPNA South Texas Chapter) or the Islamic Society of North America (ISNA) or the Islamic Council of North America (ICNA) or the Pakistan Association of Greater Houston (PAGH). Photo below is the Health Fair in 1995 at the Women’s Hospital of Texas on Fannin Street.
OFFICE GENERAL HELP: HelloRache: Our Healthcare Virtual Assistants can be connected to your current phone system and are able to make/receive calls just like they are sitting in your office. They can schedule patients, confirm appointments, call insurance companies + more. Hellorache.com (recommended by Dr. Shuja Naqvi, Houston)
This section will list major law firms that are known to defend physicians or ones physicians may need in other related matters. This is not a comprehensive list by any means but just a guide as we keep learning from other related fora.
Baker and Bott Jack Stolie andn Roser Lyles and Parker
PRE MANAGED CARE ERA: When I started solo cardiology practice in 1987, not much was heard about Managed Care in general. There was MediCare, Medicaid (Federal program for people below poverty line: patients did not have to pay anything to any provider) and then there was INDEMNITY insurance like BC BS and others which paid the provider for whatever health care service was needed on the basis of usual and customary charges. Many physicians, even in those days did not participate in MediCaid and this situation persists even today. However, there already was PruCare which was a plan of the Prudential Insurance Co and there was only one provider group called the Macgregor Clinic which held their contract. I learned for the first time what an HMO ( Health Management Organization) was; MacGregor had a HMPO contract with them meaning they were paid a fixed amount per patient and they managed the patients in that budget. Another name we heard was NYLCARE by the New York Life Insurance. We heard that they denied tests and were nicknamed DENIAL CARE! 🙂
THE ARRIVAL But the age of Managed Care had arrived. Now we had managed care companies that you had to become a member of to see their patients. That meant more paper work and several page agreements that we rarely read; it had the payment schedule as to how much we would be paid for visits and procedures and they were usually lower than what the INDEMNITY insurance. Most physicians and groups gladly signed up for them; the attraction for them was that they would be listed on the panel of those companies which would therefore give them popularity and a chance to get referrals from PCPs. Little did they realize that in signing up with them they were agreeing to their pre determined rates and could not collect any difference from the patients other than deductibles and co-pays. They would later learn that once signed up and tied to the patient volume offered by these companies, the rates would keep coming down year after year till they would become close to or even lower what MediCare paid! Now if they resigned they would lose all the volume of patients. The larger group had the wherewithal to negotiate better rates but the small groups and solos simply accepted their fate. This situation persists even today and Managed Care companies now rule the roost, requiring pre-authorizations for every procedure done in the clinic. Soon Medicare Advantage Plans would start taking over traditional Medicare from patients with promises of providing them with dental and eye coverage etc. Little do patient realize that they are giving up their freedom to choose the doctor or hospital. Fast forward from early 2000 to the 2023, these plans have grown too big for their breeches now: See the news report from November 27 2023:
Congress Increasing Scrutiny Of Medicare Advantage Plans’ Care Denials, Prior Authorization Politico (11/24, King) reported, “More than 30 million older Americans are enrolled in Medicare Advantage plans, wooed by lower premiums and more benefits than traditional Medicare offers.” However, “a bipartisan group of lawmakers is increasingly concerned that insurance companies are preying on seniors, and, in some cases, denying care that would otherwise be approved by traditional Medicare.” Congressional “scrutiny of these care denials…could have a far greater impact and reshape the rules for one of the most profitable parts of the insurance industry.” Additionally, “many physicians complain that balance has tipped too far in favor of Medicare Advantage plans.”
These and other insurance barriers have resulted over the years to increase the practice costs for the solo physician, while salaries and rents have continued to increase steadily in keeping with inflation. One or two people have to be hired to do ” pre-authorizations” for procedures, sometimes denied till the physician does a “peer to peer” review with their designated physician, often not in the same specialty.
INDEPENDENT PRACTICEORGANIZATIONS: One entity that came to the rescue of solo and small practices was the start of Physician Practice Organizations, established with the help of hospital systems; joining these provided a mechanism to negotiate payments from HMOs and PPOs as well as not having to filling forms for each company separately at times of renewal. I joined the following: Cardiovascular Care Providers St. Luke’s Independent Practice Association Methodist IPA. Gulf Coast IPA Twelve Oaks IPA The last three are closed now. The first two have been very helpful in keeping our contracts.
By Amin H. Karim MD JUNE 1987: The three year Cardiology fellowship at Baylor College of Medicine, Houston, Texas would soon end as of next month. The third year of fellowship ( as will be described in other pages) was a very busy one being on the TIMI I team along with 3 other fellows Dr. Neil Kleiman (now Director of Cath Lab at Houston Methodist Hospital), Dr. Saul Silver, and Dr. Dennis Goodman. All of us were given the third year as Interventional Fellowship on the condition that we would be the foot soldiers of the TIMI I protocol. (more on other pages)
For now the question was how best to start a private practice, having already decided that Academic job was not for me nor joining a another cardiology group. The decision to stay in Houston, Texas was already made by Shahnaz and me. The task now was to plan, budget and get started in practice. Once the Baylor job ended on June 30, 1987 I better have enough to support the family, have health insurance for family of four and other expenses. As Shahnaz was still studying for ECFMG, there was only one bread winner.
Fist step was to assess the financials condition. Luckily, I had managed to moonlight on the weekends during slower rotations. Moonlighting jobs were available in the precursors of today’s Urgent Care Centers. They were walkin clinics open from 7 AM to 11 PM. One such clinic was the MediClinic with 7 branches in Greater Houston and I would choose the one with the least traffic so that I could take my Braunwald’s Cardiology and study for the Cardiology Boards. Fellow’s salary those days was about $25,000 a year; However, cost of living was low too. Our 2 bed room apartment close to the medical center cost $350 a month. With all that there was about $4000-5000 in savings account that could be the initial cash burn in the new practice as well as living expenses.
The next stage in the strategy was to apply to about 5 neighboring hospitals for privileges. All got approved but some provisional to begin with and no procedure privileges till training was officially complete. These hospitals were: The Houston Methodist Hospital The St. Luke’s Episcopal Hospital The Medical Center Del Oro Hospital The Women’s Hospital The Park Plaza Hospital
A small 1000 square foot office was located about a mile from the Houston Methodist Hospital on South Main Street in a 5 story building. It was already built out and vacated by another physician. A dermatologist was selling all his used office furniture for $1100; Even bought a used G.E. Ecocardiogram machine from late Dr. William Gaston, a Methodist Cardiologist. I hired a front office girl for $7 an hour. All appointments and payment ledgers were on paper. Later, IMB introduced a nice PC with 20 MB of hard drive which was on sale for a whopping $3500! It came with the DOS operating system; Word or Word Perfect had to be bought separately. A program called RapidFile was used for data base accumulation like addresses and phones. Once the office was set, and come July 1, 1987 I was transformed from a fellow to a consultant or attending physician with my own office! Oh, what a feeling! 🙂 There were other paper formalities like applying for Medicaid, Medicare, Champus, BCBS and as many private insurnace
CALL COVERAGE: The next step was arranging call coverage which is a requirement for most hospitals and health care systems. I was lucky to have Dr. Mohammed Attar (originally from Syria and Lebanon) who was already in practice and was my attending during fellowship. He too was a solo practitioner and was happy to cross cover. His practice was busy so one advantage was that doing rounds for him on weekends gave me more to bill and occasionally someone would need a emergency procedure. Dr. Sarma Challa in Methodist Hospital Baytown was very busy and the only cardiologist who actually lived in Baytown. The Chapman group at Methodist Houston ( a 7 member group started by Dr. Don Chapman who was a pioneer of invasive procedures at Houston Methodist) went once a week to Baytown. Baytown did not have coronary surgery program and Dr. Challa would bring all his patients to Houston. I would cover for him during the days he could not make it to Houston ( 30 mile drive along the busy I-10). Call coverage also promoted networking and establishing relationships with established cardiologists.
But the struggle had just begun. Of all hospitals, the small Del Oro Hospital which was initially established by a group of physicians and surgeons, and later sold to HCA Systems, was the most receptive and helpful, simply because they needed new cardiologists. They had 2 already. I was fully trained in PTCA and one of the cardiologists wanted to do angioplasties but was not trained. I would scrub with him and could bill as an assistant. Later Medicare abolished assistant payments. In any case, I wanted to sharpen my angioplasty skills and would help anyone who needed my help, even at the Methodist Hospital. St. Luke’s was very strict and wanted new fellows to scrub with an established attending for 10 cases (which they would bill) as proctor before the privileges were granted. But privileges at St. Luke’s helped in another way later since Dr. Denton Cooley drew patients from Pakistan and India and some of the well known rich Pakistani industrialists became my patients. Sr. Luks’s also had a good discount rates for cash patients from abroad which Methodist lacked. Dr. Cooley in addition to being a master CV surgeon was also a good businessman and knew well how to market. I remember seeing a St. Luke’s ad in a magazine that you see in the pocket of the seat in front of you in an aircraft!
Once hospital privileges were in place, the next step was how to market oneself for referrals. The bread and butter of a consulting physician of any specialty was referrals from primary care physicians. So one method was to visit them whenever possible with cards and requisition form for test like Echo, stress tests, Holter etc. Referrals from hospital was easier since most surgeons want cardiology clearance and someone to follow on a day to day basis. I got to make friends with many good surgeons and internists. The best way I found to gain the respect of referring docs in the hospitals was to be available and affable. (as one proctor told me). Emergency room doctors were another source of great referrals of unstable angina or acute MI.
The moonlighting of course continued since even when insurances were billed, it took a few months for cheques to start rolling in. I worked at a MacGregor Clinic (now gone) which was a large multispecialty group with PruCare contract (by Prudential Insurance Co). I was paid $25 an hour for supervising treadmill stress tests. I would do 15-20 of them in a 3-4 hours and make reports. Another moonlighting job was at the West Houston Hospital at $20 an hour to take care of Surgical ICU patients and so forth. At least these jobs brought in cash at the end of the month to pay the bills and save some for visit to Pakistan.
Now for furthering the practice, one looked at the map of greater Houston and see where the smaller hospitals were in the periphery with no cardiologist coverage. I found several eg. Alvin Community Hospital (now taken over by Clear Lake Medical Center), The Angleton-Danbury Hospital, (now taken over by UTMB), the Lake Jackson Hospital (also taken over by UTMB), The BayCity Hospital, The Mainland Center Hospital in Texas City; The plan was to visit each of these hospital Emergency Rooms and make friends with the ER docs and let them know you could take acute MI patients. In those days, these hospitals would call Hermann LifeFlight or Methodist Helicopter Service and transfer the acute MI patient with or without first giving TPA. Depending on their condition we could either manage conservatively or take them straight to cath lab for rescue PTCA.
Not that it was easy to cover these distant hospitals. Once you got privileges in these places, you could be called any time of the day or night to see a consult or to read an echo. For example, Mainland Center Hospital was atleast 40 miles away from my home. Sometimes, I would be called to read a study and I would have to drive there. Now, remember we had no mobile phones then and we carried Motorola pagers for nurses to call us. If you got a call while driving on I-45 Freeway, you would have to exit the freeway and find the corner gas station. The area may not be the safest. You carried change in your car to make the phone call. Mercifully, cell phones arrived. I bought a Motorola cell phone the size of a brick which cost $2000. Twenty minutes of talk time per day was $100 per month!
More hospitals were added by me for obtaining privileges including Southeast Memorial Hospital (was not under Hermann yet), the Spring Branch Medical Center (now closed) The Sam Houston Hospital (now closed), The SunBelt Hospital (now closed due to flood destruction), At one time the toral number of hospitals and skilled nursing facilities I had privileges at numbered about 15! You can imagine rounds at these hospitals took time and would last till 11 PM.
The reward, of course, was good. There were no HMOs or PPOs. Medicare paid good for procedures. it took a couple of years ( I had been told it would) to get to a comfort zone of regular office visits, procedures, hospital admissions, consults and other work to get the practice going. Many interesting things were encountered like being approached by a attorney group to take care of a guy involved with a well known case and being a expert witness for him. (more later on that). Attorneys pay well for these cases. Also got in the cross fire of a lawsuit against a urologist when his patient died of bleeding after prostatectomy and I happened to be the cardiologist who had cleared the patient. I was, of course, non suited and later learned that the reason the lawyers get all the docs on the case involved is so they can get free expert witnesses’ when these docs try to defend themselves and inadvertently point fingers at the surgeon! There was much to learn about medico-legal medicine later in practice.
One great satisfaction was that both the Internal Medicine Boards and the Cardiology Boards were cleared in the first attempt. Later in 1999 I cleared the Interventional Cardiology Boards. Mercifully, the first two boards were grand fathered when the rules changed and were valid indefinitely and we would never have to appear in subsequent recertification. The Interventional Board expired in 10 years and I never re took it. Not that anyone cared anyone since no hospital took my interventional privileges away as long as I was actively admitting to the hospital. I still take STEMI calls.
In 1981-84 I was a resident at the Sinai Hospital of Baltimore, Maryland. Dr. Joseph Solomon was a cardiologist and the CCU attending and the only invasive cardiologist in the hospital; he did only left and right heart catheterizations. Patients needing coronary intervention were sent to either Johns Hopkins downtown Baltimore or to Minnesota to Dr. Dudley Johnson. I took care of a patient with heart failure symptoms which turned out to be constrictive pericarditis. The case was reported and published in the American Journal of Medicine in 1985. Amin H. Karim MD