Asli Hacioglu MD
Gazi University, Ankara, Turkey

and
Hareesha Rishab MBBS, National Health Service, United Kingdom
Amin H. Karim MD, Baylor College of Medicine, Houston, Texas and Institute for Academic Medicine, Houston, Texas

Asli Hacioglu MD
Gazi University, Ankara, Turkey
and
Hareesha Rishab MBBS, National Health Service, United Kingdom
Amin H. Karim MD, Baylor College of Medicine, Houston, Texas and Institute for Academic Medicine, Houston, Texas
By
Ajala GLoria Eyitayo
All Saints University School of Medicine
Diego Gomez de la Garza
Universidad de Monterrey, Mexico
Amin H. Karim MD
Baylor College of Medicine
Houston, Texas

By Jessica Eve (Java, Indonesia)
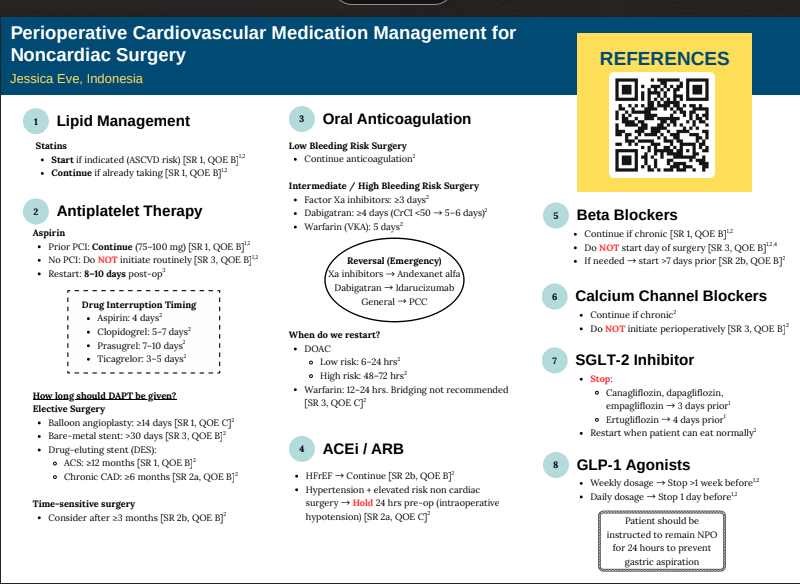
REFERENCES
Heart Failure with Preserved Ejection Fraction and Atrial
Fibrillation: What was first, the Egg or the Chicken?
Laiba Ejaz
Karachi Institute of Medical Sciences.
Samuel Sotelo Hernandez
Autonomous University of Durango-Cappus Zacatecas
Amin H. Karim MD
Methodist Academy of Medicine, Houston, Texas
Abstract
A 68-year-old African American man presented with recurrent lower extremity edema without dyspnea or chest pain. His history included hypertension, hyperlipidemia, and obesity. Evaluation revealed atrial fibrillation with a
controlled ventricular rate and echocardiographic findings consistent with heart failure with preserved ejection fraction (HFpEF). Secondary causes such as deep venous thrombosis were excluded. The patient was managed
with metoprolol and diuretics for rate and volume control, losartan and hydrochlorothiazide for hypertension, apixaban for anticoagulation, and amiodarone for rhythm stabilisation. After a year of persistent atrial
fibrillation, elective cardioversion successfully restored sinus rhythm following confirmation of the absence of atrial thrombus on transesophageal echocardiography. The patient remained clinically stable on subsequent
follow-up visits.
Introduction
Atrial fibrillation (AF) and heart failure with preserved ejection fraction (HFpEF) are common cardiovascular conditions that frequently coexist, particularly in older, hypertensive, and obese patients. AF can exacerbate
HFpEF by impairing atrial contribution to ventricular filling, while HFpEF may predispose to atrial remodelling and subsequent arrhythmia, creating a complex bidirectional relationship. Both conditions independently
increase morbidity and mortality and pose challenges in diagnosis and management, especially when symptoms such as edema or fatigue are subtle or overlapping. Understanding the temporal relationship between AF and
HFpEF is critical for optimizing therapy, including rate versus rhythm control, anticoagulation, and management of comorbidities. This case highlights a patient with recurrent lower extremity edema, AF, and HFpEF, raising
the clinical question of which condition preceded the other and illustrating the importance of individualized, comprehensive cardiovascular care.
Case Presentation
A 68-year-old African American man presented to the clinic with complaints of recurrent fluid buildup, mainly in his lower extremities, as noted by his primary care physician. He denied dyspnea, chest pain, orthopnea, or
paroxysmal nocturnal dyspnea. His medical history included hypertension, hyperlipidemia, and obesity. He reported occasional alcohol use and denied smoking. His family history was significant for coronary artery
disease, hypertension, hyperlipidemia, and diabetes mellitus. On examination, his weight was 280 lbs (127 kg) and height 73 inches, yielding a BMI of 37.7 kg/m2, consistent with Class I obesity. Blood pressure ranged
between 135–145/75–85 mmHg, and his pulse was irregular at 58–70 beats per minute.
Laboratory
investigations revealed a normal HbA1c and a lipid profile with total cholesterol 222 mg/dL, HDL 67 mg/dL, LDL 149 mg/dL, and triglycerides 60 mg/dL. An electrocardiogram (EKG) (figure 1) obtained during the initial
visit showed atrial fibrillation with a controlled ventricular rate of approximately 58 beats per minute. A subsequent 2D echocardiogram demonstrated a preserved left ventricular ejection fraction of 60–65% and mild
left atrial enlargement—findings consistent with heart failure with preserved ejection fraction (HFpEF). Chest X-ray showed chronic airway changes and mild atherosclerosis, while Doppler ultrasound ruled out deep
venous thrombosis. The patient was started on metoprolol and diuretics for rate and volume control, along with losartan and hydrochlorothiazide for blood pressure management. Anticoagulation with Eliquis (apixaban) and
rhythm control with amiodarone was initiated and continued for over a year without spontaneous conversion to sinus rhythm (figure 2). He subsequently underwent elective cardioversion, which successfully restored sinus
rhythm (figure 3) A transesophageal echocardiogram prior to the procedure confirmed the absence of thrombus in the left atrium or left atrial appendage. The patient continued regular follow-up and remained clinically stable
thereafter.
Discussion
This case highlights the complex interplay between atrial fibrillation (AF), hypertension, obesity, and heart failure with preserved ejection fraction (HFpEF) in an older African American male. The patient’s presentation
with peripheral edema, in the absence of dyspnea or orthopnea, emphasises that HFpEF can manifest subtly and that careful evaluation of cardiovascular risk factors and cardiac rhythm is essential for accurate diagnosis and
management (1,2). Atrial fibrillation is a common arrhythmia in elderly individuals, often associated with structural heart changes such as left atrial enlargement and diastolic dysfunction. In this patient, chronic
hypertension and obesity likely contributed to increased left ventricular stiffness and impaired relaxation, leading to diastolic dysfunction and, consequently, HFpEF (3,4). The echocardiographic findings of preserved left
ventricular ejection fraction (60–65%) with mild left atrial enlargement are consistent with this diagnosis. The irregularly irregular rhythm on electrocardiogram confirmed the presence of AF, while the controlled ventricular rate suggested adequate rate control with beta-blocker therapy (5).
HFpEF accounts for nearly half of all heart failure cases, and its prevalence continues to rise in parallel with obesity, hypertension, and metabolic syndrome (1,6). Pathophysiologically , the combination of increased
ventricular wall stress, endothelial dysfunction, and myocardial fibrosis results in elevated filling pressures despite normal systolic function (7). This leads to symptoms such as lower extremity edema, exercise intolerance, or mild dyspnea, which may fluctuate depending on volume status. Importantly, obesity is a key modifiable factor that exacerbates both HFpEF and AF by promoting systemic inflammation, left atrial remodelling, and neurohormonal activation (6,7). The management of this patient was appropriately focused on
controlling heart rate, optimizing blood pressure, managing volume status, and preventing thromboembolic events. Beta-blocker therapy (metoprolol) was effective for rate control, while diuretics addressed the peripheral
edema. Losartan and hydrochlorothiazide provided additional blood pressure control and diuresis. Given the patient’s CHA2DS2-VASc score—elevated due to age, hypertension, and heart failure—anticoagulation with
apixaban was warranted to reduce the risk of stroke, which is fivefold higher in individuals with AF (5,8). Despite more than a year of rate control and anticoagulation, the patient did not experience spontaneous
reversion to sinus rhythm. Therefore, elective cardioversion was pursued, preceded by transesophageal echocardiography to rule out intracardiac thrombus. The successful restoration of sinus rhythm improved cardiac
efficiency and potentially reduced the risk of HF progression (9). Ongoing rhythm surveillance is essential, as recurrence of AF is common, particularly in patients with underlying structural heart disease and obesity (10).
From a preventive perspective, aggressive risk factor modification remains a cornerstone of long -term management. Weight reduction, dietary sodium restriction, and increased physical activity can improve diastolic
function and reduce AF recurrence (1,2). Additionally, lipid lowering with statin therapy is indicated given the elevated LDL cholesterol level (149 mg/dL), further reducing cardiovascular risk (3,6).
In summary, this case underscores the importance of a multidisciplinary approach in managing AF and HFpEF , particularly in patients with multiple cardiovascular risk factors. Optimal control of hypertension, obesity, and
dyslipidemia, combined with rhythm management and anticoagulation, can lead to favorable clinical outcomes. The patient’s successful cardioversion and stable follow-up course demonstrate that with comprehensive care,
symptom control and maintenance of sinus rhythm are achievable in this complex patient population.
References:
from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12502451/
By
Ana María Sierra Valiente Universidad Anáhuac México Norte
Amin H. Karim MD,
Clinical Associate Professor
Baylor College of Medicine, Houston, Texas.

Amin H. Karim MD
Houston Methodist Academic Institute
and Weill Medical College of
Dear Dentist: My Murmur Doesn’t Need Meds Anymore!
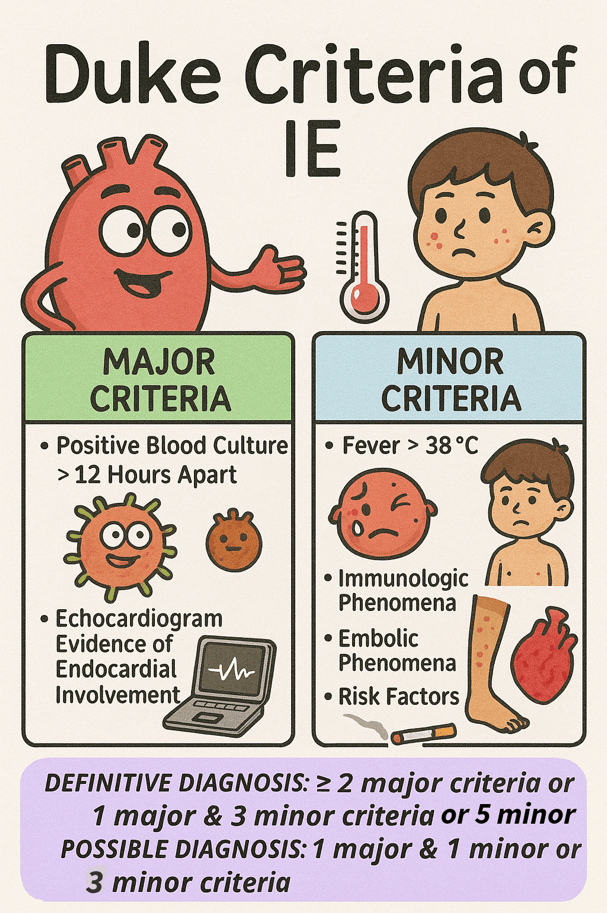
Infective endocarditis (IE) is a serious infection of the heart’s inner lining, affecting 3 to 10 people per 100,000 annually. It carries a significant risk, with mortality reaching up to 30% within the first 30 days 1 . Staphylococcus aureus was the most frequently identified pathogen, accounting for 31% of cases. The mitral valve was the most commonly affected, involved in forty-one percent of infections, while the aortic valve was affected in thirty-eight percent of cases 2. The diagnosis of IE is primarily clinical and is based on the modified Duke criteria, which include a combination of major and minor clinical, microbiological, and echocardiographic findings.
Guntheroth et al. observed that bacteremia was present in 40% of 2,403 cases following tooth extraction, 38% of individuals during routine mastication, and 11% of those with oral sepsis in the absence of any dental intervention 3. This issue has long concerned both dentists and cardiologists, driven in part by a preference for commission bias—favoring action over inaction—when considering prophylactic antibiotic use.
American Heart Association revised the guidelines on infective endocarditis prophylaxis in 2007 (full guidelines available at http://circ.ahajournals.org ) to promote the judicious use of antibiotics, particularly in clinical scenarios where the anticipated benefits are outweighed by the risks, such as the emergence of antibiotic resistance and the potential for adverse drug reactions. The present revised document was not based on the results of a single study but rather on the collective body of evidence published in numerous studies over the past two decades. The following points were used as a rationale by AHA for updating the guideline4.
Several studies have demonstrated that the lifetime risk of infective endocarditis (IE) varies significantly depending on the underlying cardiac condition. In the general population without known heart disease, the risk is approximately 5 cases per 100,000 patient-years. Patients with rheumatic heart disease (RHD) face a substantially higher risk, ranging from 380 to 440 cases per 100,000 patient-years, which is comparable to the risk observed in individuals with mechanical or bioprosthetic heart valves (308 to 383 cases per 100,000 patient-years)5 .
The greatest risks are observed in the following groups:
These variations in risk highlight the importance of tailoring preventive measures to individual patient profiles.
Further research indicates that even with perfect effectiveness, antibiotic prophylaxis would prevent only a negligible number of infective endocarditis cases—given that the estimated absolute risk after a dental procedure is about 1 in 1.1 million for mitral valve prolapse, 1 in 475 000 for congenital heart disease, 1 in 142 000 for rheumatic heart disease, 1 in 114 000 for prosthetic heart valves, and 1 in 95 000 for those with a history of endocarditis6 7 .
Cardiac Conditions Associated with the Highest Risk of Adverse Outcome from Endocarditis for Which Prophylaxis Is Reasonable
Guidelines also clearly stated that antibiotic prophylaxis is no longer recommended for any other form of congenital heart disease which explicitly includesheart murmurs, valvular regurgitation, or stenosis without prosthetic material or prior endocarditis 4.
Preventing Infective Endocarditis: Procedures Requiring Antimicrobial Prophylaxis
High-Risk Procedures Requiring Antibiotic Prophylaxis
Low-Risk Procedures Not Requiring Antibiotic Prophylaxis
Infective Endocarditis Prophylaxis: Antibiotic Recommendations
Considering rising antimicrobial resistance and the potential for Clostridioides difficile infection linked to antibiotic use, it is advised against relying on the outdated “better safe than sorry” approach to prophylactic antibiotic use, as it may cause more harm than benefit to patients.
References
1. Mostaghim AS, Lo HYA, Khardori N. A retrospective epidemiologic study to define risk factors, microbiology, and clinical outcomes of infective endocarditis in a large tertiary-care teaching hospital. SAGE Open Med. 2017;5. doi:10.1177/2050312117741772
2. Murdoch DR. Clinical Presentation, Etiology, and Outcome of Infective Endocarditis in the 21st Century. Arch Intern Med. 2009;169(5):463. doi:10.1001/archinternmed.2008.603
3. Guntheroth WG. How important are dental procedures as a cause of infective endocarditis? Am J Cardiol. 1984;54(7):797-801. doi:10.1016/S0002-9149(84)80211-8
4. Wilson W, Taubert KA, Gewitz M, et al. Prevention of Infective Endocarditis. Circulation. 2007;116(15):1736-1754. doi:10.1161/CIRCULATIONAHA.106.183095
5. Steckelberg JM; WWR. Risk factors for infective endocarditis. Infectious disease clinics of North America. 1993;7(1):9-19.
6. Pallasch TJ, Wahl MJ. Focal infection: new age or ancient history? Endod Topics. 2003;4(1):32-45. doi:10.1034/j.1601-1546.2003.00002.x
7. Pallasch TJ. Antibiotic prophylaxis: problems in paradise. Dent Clin North Am. 2003;47(4):665-679. doi:10.1016/S0011-8532(03)00037-5
8. Ward RC, McGill T, Adel F, et al. Infection Rate and Outcomes of Watchman Devices: Results from a Single-Center 14-Year Experience. Biomed Hub. 2021;6(2):59-62. doi:10.1159/000516400
9. Canpolat U. Tailored antibiotic prophylaxis in patients undergoing CIED implantation: One size does not fit all the principle. Pacing and Clinical Electrophysiology. 2019;42(4):483-483. doi:10.1111/pace.13624
10. Tanabe Y, Sato Y, Izumo M, et al. Endothelialization of an Amplatzer Septal Occluder Device 6 Months Post Implantation: Is This Enough Time? An In Vivo Angioscopic Assessment. Journal of Invasive Cardiology. 2019;31(2). doi:10.25270/jic/18.00206
