Asli Hacioglu MD
Gazi University, Ankara, Turkey

and
Hareesha Rishab MBBS, National Health Service, United Kingdom
Amin H. Karim MD, Baylor College of Medicine, Houston, Texas and Institute for Academic Medicine, Houston, Texas

Asli Hacioglu MD
Gazi University, Ankara, Turkey
and
Hareesha Rishab MBBS, National Health Service, United Kingdom
Amin H. Karim MD, Baylor College of Medicine, Houston, Texas and Institute for Academic Medicine, Houston, Texas
By
Ajala GLoria Eyitayo
All Saints University School of Medicine
Diego Gomez de la Garza
Universidad de Monterrey, Mexico
Amin H. Karim MD
Baylor College of Medicine
Houston, Texas
Students are given opportunity to study a case and write up a talk for the other students:




Students from Nigeria, Pakistan, Mexico, India, Nepal. 2026.

Observers from Turkey, Mexico, USA, Indonesia. April 2026

By Jessica Eve (Java, Indonesia)
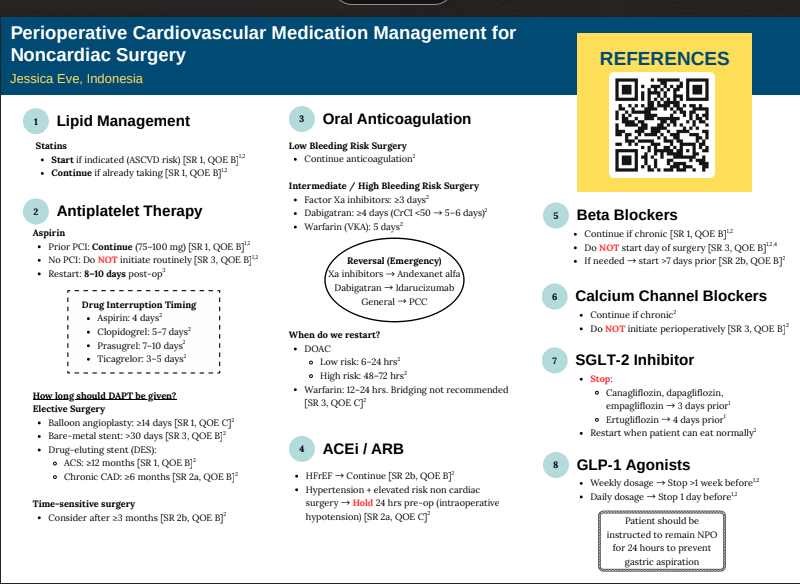
REFERENCES
Heart Failure with Preserved Ejection Fraction and Atrial
Fibrillation: What was first, the Egg or the Chicken?
Laiba Ejaz
Karachi Institute of Medical Sciences.
Samuel Sotelo Hernandez
Autonomous University of Durango-Cappus Zacatecas
Amin H. Karim MD
Methodist Academy of Medicine, Houston, Texas
Abstract
A 68-year-old African American man presented with recurrent lower extremity edema without dyspnea or chest pain. His history included hypertension, hyperlipidemia, and obesity. Evaluation revealed atrial fibrillation with a
controlled ventricular rate and echocardiographic findings consistent with heart failure with preserved ejection fraction (HFpEF). Secondary causes such as deep venous thrombosis were excluded. The patient was managed
with metoprolol and diuretics for rate and volume control, losartan and hydrochlorothiazide for hypertension, apixaban for anticoagulation, and amiodarone for rhythm stabilisation. After a year of persistent atrial
fibrillation, elective cardioversion successfully restored sinus rhythm following confirmation of the absence of atrial thrombus on transesophageal echocardiography. The patient remained clinically stable on subsequent
follow-up visits.
Introduction
Atrial fibrillation (AF) and heart failure with preserved ejection fraction (HFpEF) are common cardiovascular conditions that frequently coexist, particularly in older, hypertensive, and obese patients. AF can exacerbate
HFpEF by impairing atrial contribution to ventricular filling, while HFpEF may predispose to atrial remodelling and subsequent arrhythmia, creating a complex bidirectional relationship. Both conditions independently
increase morbidity and mortality and pose challenges in diagnosis and management, especially when symptoms such as edema or fatigue are subtle or overlapping. Understanding the temporal relationship between AF and
HFpEF is critical for optimizing therapy, including rate versus rhythm control, anticoagulation, and management of comorbidities. This case highlights a patient with recurrent lower extremity edema, AF, and HFpEF, raising
the clinical question of which condition preceded the other and illustrating the importance of individualized, comprehensive cardiovascular care.
Case Presentation
A 68-year-old African American man presented to the clinic with complaints of recurrent fluid buildup, mainly in his lower extremities, as noted by his primary care physician. He denied dyspnea, chest pain, orthopnea, or
paroxysmal nocturnal dyspnea. His medical history included hypertension, hyperlipidemia, and obesity. He reported occasional alcohol use and denied smoking. His family history was significant for coronary artery
disease, hypertension, hyperlipidemia, and diabetes mellitus. On examination, his weight was 280 lbs (127 kg) and height 73 inches, yielding a BMI of 37.7 kg/m2, consistent with Class I obesity. Blood pressure ranged
between 135–145/75–85 mmHg, and his pulse was irregular at 58–70 beats per minute.
Laboratory
investigations revealed a normal HbA1c and a lipid profile with total cholesterol 222 mg/dL, HDL 67 mg/dL, LDL 149 mg/dL, and triglycerides 60 mg/dL. An electrocardiogram (EKG) (figure 1) obtained during the initial
visit showed atrial fibrillation with a controlled ventricular rate of approximately 58 beats per minute. A subsequent 2D echocardiogram demonstrated a preserved left ventricular ejection fraction of 60–65% and mild
left atrial enlargement—findings consistent with heart failure with preserved ejection fraction (HFpEF). Chest X-ray showed chronic airway changes and mild atherosclerosis, while Doppler ultrasound ruled out deep
venous thrombosis. The patient was started on metoprolol and diuretics for rate and volume control, along with losartan and hydrochlorothiazide for blood pressure management. Anticoagulation with Eliquis (apixaban) and
rhythm control with amiodarone was initiated and continued for over a year without spontaneous conversion to sinus rhythm (figure 2). He subsequently underwent elective cardioversion, which successfully restored sinus
rhythm (figure 3) A transesophageal echocardiogram prior to the procedure confirmed the absence of thrombus in the left atrium or left atrial appendage. The patient continued regular follow-up and remained clinically stable
thereafter.
Discussion
This case highlights the complex interplay between atrial fibrillation (AF), hypertension, obesity, and heart failure with preserved ejection fraction (HFpEF) in an older African American male. The patient’s presentation
with peripheral edema, in the absence of dyspnea or orthopnea, emphasises that HFpEF can manifest subtly and that careful evaluation of cardiovascular risk factors and cardiac rhythm is essential for accurate diagnosis and
management (1,2). Atrial fibrillation is a common arrhythmia in elderly individuals, often associated with structural heart changes such as left atrial enlargement and diastolic dysfunction. In this patient, chronic
hypertension and obesity likely contributed to increased left ventricular stiffness and impaired relaxation, leading to diastolic dysfunction and, consequently, HFpEF (3,4). The echocardiographic findings of preserved left
ventricular ejection fraction (60–65%) with mild left atrial enlargement are consistent with this diagnosis. The irregularly irregular rhythm on electrocardiogram confirmed the presence of AF, while the controlled ventricular rate suggested adequate rate control with beta-blocker therapy (5).
HFpEF accounts for nearly half of all heart failure cases, and its prevalence continues to rise in parallel with obesity, hypertension, and metabolic syndrome (1,6). Pathophysiologically , the combination of increased
ventricular wall stress, endothelial dysfunction, and myocardial fibrosis results in elevated filling pressures despite normal systolic function (7). This leads to symptoms such as lower extremity edema, exercise intolerance, or mild dyspnea, which may fluctuate depending on volume status. Importantly, obesity is a key modifiable factor that exacerbates both HFpEF and AF by promoting systemic inflammation, left atrial remodelling, and neurohormonal activation (6,7). The management of this patient was appropriately focused on
controlling heart rate, optimizing blood pressure, managing volume status, and preventing thromboembolic events. Beta-blocker therapy (metoprolol) was effective for rate control, while diuretics addressed the peripheral
edema. Losartan and hydrochlorothiazide provided additional blood pressure control and diuresis. Given the patient’s CHA2DS2-VASc score—elevated due to age, hypertension, and heart failure—anticoagulation with
apixaban was warranted to reduce the risk of stroke, which is fivefold higher in individuals with AF (5,8). Despite more than a year of rate control and anticoagulation, the patient did not experience spontaneous
reversion to sinus rhythm. Therefore, elective cardioversion was pursued, preceded by transesophageal echocardiography to rule out intracardiac thrombus. The successful restoration of sinus rhythm improved cardiac
efficiency and potentially reduced the risk of HF progression (9). Ongoing rhythm surveillance is essential, as recurrence of AF is common, particularly in patients with underlying structural heart disease and obesity (10).
From a preventive perspective, aggressive risk factor modification remains a cornerstone of long -term management. Weight reduction, dietary sodium restriction, and increased physical activity can improve diastolic
function and reduce AF recurrence (1,2). Additionally, lipid lowering with statin therapy is indicated given the elevated LDL cholesterol level (149 mg/dL), further reducing cardiovascular risk (3,6).
In summary, this case underscores the importance of a multidisciplinary approach in managing AF and HFpEF , particularly in patients with multiple cardiovascular risk factors. Optimal control of hypertension, obesity, and
dyslipidemia, combined with rhythm management and anticoagulation, can lead to favorable clinical outcomes. The patient’s successful cardioversion and stable follow-up course demonstrate that with comprehensive care,
symptom control and maintenance of sinus rhythm are achievable in this complex patient population.
References:
from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12502451/
In 1977 I wrote up a small booklet called CLINICAL STUDENTS COMPANION and had it published by AzamSons, a book seller across from Dow Medical College. It was basically notes on General Medicine I made for the Final Professional MBBS Exam. It was common for oral examiners to ask for causes of symptoms, signs or abnormal lab values. This helped junior students to brush up on lists of causes which one could not find easily from text books of Medicine like Davidson or Harrison or Cecil Loeb. I then published two more editions wht last one being what is being uploaded here, a 260 page book with illustrations. The third edition was typed by me on the old manual Smith Corona portable type-writer.
One technique we learnt from teachers like Prof. S.M Rab (with whom I did my first intership in Medicine at Jinnah PostGraduate Medical Center, Karachi) was to think about the causes of a presentation or symptom or sign one at a time. If patient has 2-4 signs think of all the causes separately and try to figure what runs common to all the lists. This may lead one to correct diagnosis. For example when presented with Fever of Unknown Origin, think of the causes and if the patient also has anemia and splinter hemorrhages, one would find that bacterial endocarditis is present in all the 3 lists. Same for other problems.
Hope you enjoy reading. Mind you this is 45 years ago and applies to diseases found commonly in Pakistan and India. It’s value at this stage may be more historical than actual since everything now is a mouse click away on ChatGPT! 🙂 Amin H. Karim MD September 25 2025
A CASE OF POSTOPERATIVE COMPLICATION OF SURGICAL MITRAL VALVE REPLACEMENT.
Amin H. Karim MD
CASE:
A 71 year olf Caucasian male with history of hypertension and hyperlipidemia, and chronic atrial fibrillation, developed non-rheumatic mitral valve regurgitation secondary to mitral valve prolapse, which had gradually progressed over a decade years to severe regurgitation, accompanied by moderately severe tricuspid regurgitation. Patient tolerated the valvular lesions for many years till he became symptomatic with NYHA Class III dyspnea and agreed for intervention.
CARDIAC MRI: In November 2024, cardiac MRI revealed bi-leaflet mitral valve prolapse, with severe left atrial enlargement and moderate tricuspid regurgitation. The global ejection fraction was 65% with biventricular dilatation, and basal and mid inferolateral wall scarring. Mitral and tricuspid annulus were dilated.
TWO DIMENSIONAL ECHOCARDIOGRAM: On Echocardiogram, right ventricular function was low normal. Left ventricular ejection fraction was normal. There was mitral valve prolapse due to myxomatous degeneration, severe mitral regurgitation with regurgitation fraction of 51% and estimated regurgitant volume of 56 ml. Pulmonary artery pressures were normal. Cardiac catheterization showed normal coronaries
With a low BMI and good overall health, he was felt by the cardiovascular surgeon to be low risk for surgery and MitraClip therefore not warranted.
MITRAL VALVE REPAIR SURGERY:
Mitral valve repair with a 34 mm physio 2 flexible annuloplasty ring; Intra-aortic balloon pump; Tricuspid valve repair with a 28 mm triad rigid ring; Biatrial maze utilizing the encompass clamp, RF clamp and cryoprobe; Left atrial appendage ligation with a 45 mm atrial cure mini atrial clip:
Following mitral valve repair there was no mitral regurgitation with a long segment of coaptation beneath the annular plane. The transmitral gradient was 1 mm Hg. Similarly following tricuspid valve repair there was no regurgitation with the trans tricuspid valve gradient of 1 mm.
Following bi-atrial maze procedure, the patient converted to sinus rhythm. However, when the cardio pulmonary bypass was reversed and the patient was being closed, he went to ventricular fibrillation followed by defibrillation. Frequent PVCs were observed. Intravenous amiodarone and magnesium were started; His blood pressure started to drop and vasopressors were increased and intra-aortic balloon placed. His hemodynamics improved and was watched in the OR with echo. There was inferior wall hypokinesis. He was maintained on low dose dobutamine, vasopressin and norepinephrine. His global ejection fraction was reasonable; chest was closed, but before he could be transferred out of OR he developed ventricular fibrillation again. His chest was opened and direct cardiac massage and cardioversion done with return of circulation. ECMO (Extracorporeal Membrane Oxygenation) was initiated. He was transferred to the cardiac cath lab and underwent emergency coronary angiography.
CORONARY INTERVENTION: Coronary angiography showed the dominant left circumflex was occluded in the mid potion.
IVUS showed possible edema around the left circumflex and it was felt that the circumflex was occluded due to pressure from the mitral valve ring. Stent was placed with recanalization. Impella was placed in the cath lab and the intra-aortic balloon was removed.
Intavascular Ultrasound (IVUS) shows the edema/hematoma? aeound the left vircumflex artery.
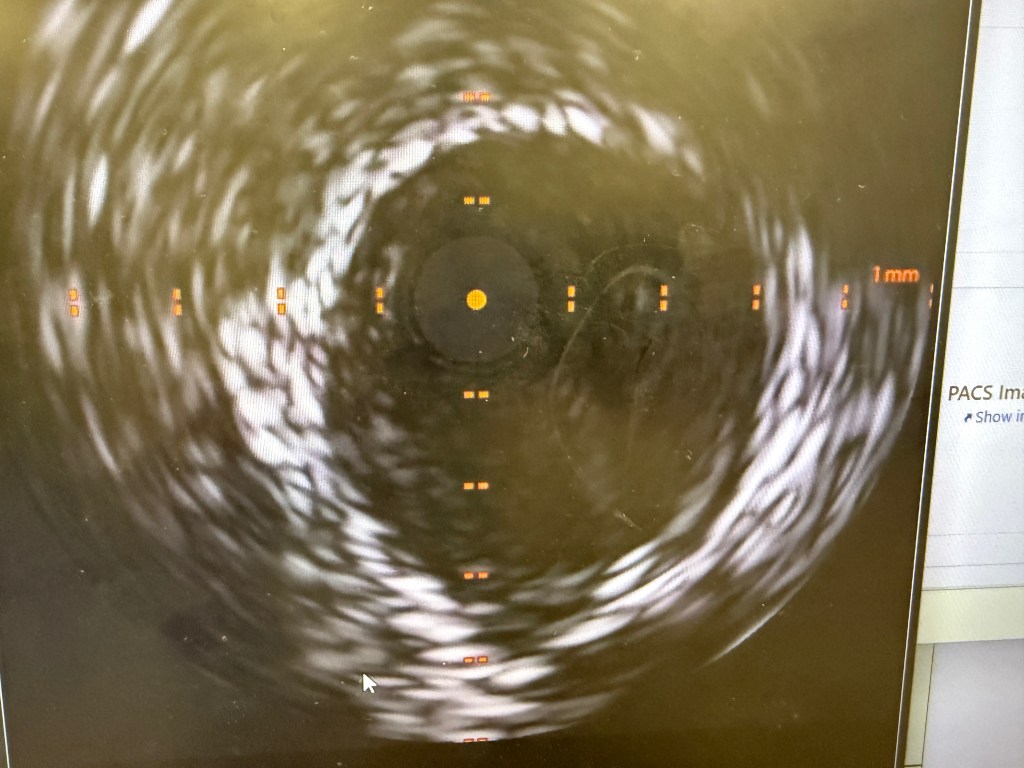
A 3.5 mm x 32 mm Synergy drug eluting stent was placed in the mid circumflex coronary artery with a good result. The intra-aortic balloon was removed.
INTENSIVE CARE UNIT: Patient remained with supported blood pressure, with severe anemia needing multiple blood transfusions. Transesophageal echo showed severely depressed right and left ventricular systolic function.
Patient was taken back to O.R. for exploration and washout. On return to ICU noted to have ST elevation in lead VII. Taken back to cath lab and coronary angiography done showing that the circumflex stent was patent.
FOLLOWUP: 10 days after mitral and tricuspid valve repair and coronary intervention, patient is off ECMO, and on Impella support. He is awake but does not follow commands. His global ejection fraction on echocardiogram is mildly depressed (40-45%) with trace of mitral and tricuspid regurgitation.
Authors:
Ana Maria Sierra Valiente
Universidad Anahuac Mexico Norte
Joy Emem Efik, MBBS
Sumy State University
Ayesha Asghar, MBBS
Multan Medical and Dental College, Pakistan.
Sarai Anayansi Zárate Chavez
Universidad Anahuac Oaxaca
Amin H. Karim MD, FRCP
Baylor College of Medicine, Houston
Academy of Medicine, Houston
Weill Medical College of Cornell University.
By
Ana María Sierra Valiente Universidad Anáhuac México Norte
Amin H. Karim MD,
Clinical Associate Professor
Baylor College of Medicine, Houston, Texas.
Interrupting Anticoagulants for Surgery: Guidelines, Risk Stratification, and Clinical Decision-Making.
Raya Kharboutli PA-S2
University of Texas Medical Branch

Regina Medina Urrutia
Universidad Anahuac Campus Xalapa

Anticoagulants are a class of medications used to prevent and treat thromboembolic events such as stroke, deep vein thrombosis, and pulmonary embolism. These agents are divided into two main categories: antiplatelet agents and anticoagulants that inhibit coagulation factors. Understanding their mechanisms of action is critical for making safe perioperative decisions.
Antiplatelet agents like aspirin irreversibly inhibit cyclooxygenase (COX-1), preventing the production of thromboxane A₂, a molecule essential for platelet activation. As a result, platelet aggregation is impaired for the lifespan of the platelet, which is approximately 7-9 days (1). Clopidogrel, a P2Y12 receptor inhibitor, irreversibly blocks ADP receptors on the platelet surface, further preventing platelet activation and aggregation. Following discontinuation, platelet function typically returns to baseline within about 5 days (2). Warfarin is a vitamin K antagonist that works by inhibiting vitamin K epoxide reductase, an enzyme required for the activation of clotting factors II, VII, IX, and X. Warfarin has a delayed onset of action, with therapeutic anticoagulation typically achieved within 2 to 3 days. Monitoring is performed using International Normalized Ratio (INR), and full reversal of anticoagulant effect takes approximately 3 to 5 days. This process can be expedited with the administration of vitamin K (3). Direct oral anticoagulants (DOACs) are a newer class of medications with more predictable pharmacokinetics. These include factor Xa inhibitors such as apixaban, rivaroxaban, and edoxaban, which inhibit factor Xa, thereby blocking the conversion of prothrombin to thrombin. Additionally, dabigatran is a direct thrombin inhibitor (Factor IIa), which prevents the conversion of fibrinogen to fibrin, the final step in clot formation (4).
The type of anticoagulant used plays an important role in how far in advance it should be discontinued:
This classification and understanding of mechanisms provide a foundation for evaluating how and when these agents should be temporarily discontinued prior to surgical or invasive procedures, based on the individual agent, patient thrombotic risk, and the bleeding risk associated with the procedure
Interrupting anticoagulation before a procedure is often necessary to reduce the risk of excessive bleeding during or after surgery. Anticoagulants and antiplatelet agents impair the body’s ability to form clots, which is beneficial for preventing thrombosis but can lead to significant complications when tissue trauma or vascular injury is expected. The decision to pause these medications is a balance between two major risks: bleeding and thrombosis. For procedures with a high bleeding risk, such as major surgeries, spinal or epidural anesthesia, and certain endoscopic or urologic procedures, continued anticoagulation can increase the chance of uncontrolled bleeding, hematoma formation, or the need for transfusions (5). On the other hand, abruptly stopping antithrombotic therapy, especially in high-risk patients (such as those with recent stroke, atrial fibrillation, or coronary stents), may raise the risk of life-threatening thromboembolic events (7). Therefore, clinicians must evaluate the type of anticoagulant, the patient’s thrombotic risk, and the bleeding risk of the procedure to determine the safest perioperative plan. In many cases, temporary interruption with or without bridging therapy allows for safe procedural outcomes while minimizing harm from both bleeding and clot formation (6).
In cardiology, several invasive procedures carry moderate to high bleeding risk and typically require temporary interruption of anticoagulant or antiplatelet therapy. The decision depends on the type of medication, the procedure’s bleeding risk, and the patient’s thromboembolic risk. For cardiac surgery, such as coronary artery bypass grafting (CABG) or valve replacement, both antiplatelet agents and anticoagulants are usually interrupted. Aspirin is often continued unless bleeding risk is very high but clopidogrel is typically discontinued at least 5-7 days before surgery to minimize perioperative bleeding (8). Warfarin is usually stopped 5 days prior, aiming for an INR of less than 1.5 on the day of the surgery. In patients at high thromboembolic risk such as mechanical valve or atrial fibrillation with prior stroke, bridging with low molecular weight heparin (LMWH) may be considered. Direct oral anticoagulants are typically held for 2-3 days before major cardiac surgery, with the exact timing depending on renal function.
For pacemaker or implantable cardioverter-defibrillator (ICD) insertion, the bleeding risk is considered moderate. Aspirin may be continued in most cases, but clopidogrel should be stopped 5-7 days prior, especially if dual antiplatelet therapy is not mandatory at the time. DOACs are commonly interrupted 24-48 hours before the procedure, depending on renal function and Warfarin is often continued at a therapeutic INR for minor device procedures, but only interrupted in high-bleeding-risk cases (9). Percutaneous coronary intervention (PCI) presents a unique challenge, especially in patients already on dual antiplatelet therapy (DAPT). These procedures are rarely elective if DAPT is indicated. If non-urgent PCI must be delayed, clopidogrel is held 5-7 days and DOACs for 48-72 hours prior (10).
Ultimately, the goal is to minimize both bleeding and thrombotic complications by tailoring medication interruption based on the procedure type, medication half-life, and patient risk factors.
The management of patients going under anesthesia for surgery is a really common challenge due to the decision to suspend or not the anticoagulants the patients are on. Many protocols can be followed to help make the decision. One of these protocols is to evaluate both the risk of bleeding and thromboembolism, and it’s important to know the dosage of the anticoagulant and the reasons why the patient is taking the specific anticoagulant.
First of all, the risk of bleeding needs to be estimated. One way is the HAS-BLEED score, which will assess the following risk factors such as hypertension, abnormal liver or renal functions, stroke, bleeding, labile INRs, elderly patients (>65 years), and the use of drugs or alcohol. The second step is to estimate the thromboembolic risk, and to do that, age and comorbidities need to be evaluated (12). If the patient has had a recent event of DVT or PE, the decision is based on the diagnosis, but in this scenario, the surgery is delayed as much as possible. Once the two important risks are evaluated, the duration to interrupt the anticoagulant is going to depend on which medication the patient is on. If the patient has low kidney or liver function, we might need additional consideration. In general, almost every procedure, the anticoagulant must be suspended if the risk of bleeding or high thrombotic risk, but if the risk is low isn’t necessarily necessary to stop the medication (12).
There are really selected procedures where we can keep using the anticoagulant, like in a dental extraction, skin biopsy, or a cataract surgery, but also in a procedure like a cardiac implant electronic device, it’s not necessary to stop taking them. The ERHA states that if the patient is going to be under the implantation of a cardiac electronic device like a pacemaker, the patient should continue the anticoagulant perioperatively (13). Unless the patient has a risk of a thromboembolic event and is under warfarin or DOCAs, the medication should be suspended temporarily. In the case of any endovascular procedures like an angioplasty, a meta-analysis randomly shows that patients who were under warfarin and didn’t interrupt while undergoing the procedure were associated with lower risks of complications compared with those who interrupted the warfarin perioperatively (11).
In patients with high thrombotic risk, it may be necessary to use bridging therapy with low-molecular-weight heparin (LMWH) during the time the oral anticoagulant is stopped. However, the BRIDGE trial showed that bridging in patients with non-valvular atrial fibrillation and moderate thrombotic risk increased the risk of bleeding without significantly reducing thromboembolic events (14). Therefore, bridging should only be considered in selected high-risk patients.
When using spinal or epidural anesthesia, anticoagulants increase the risk of spinal hematoma, which can cause permanent paralysis. According to the American Society of Regional Anesthesia (ASRA), anticoagulants such as DOACs should be stopped at least 72 hours before any neuraxial procedures, and specific guidelines should be followed for restarting the medication (15).
Individual characteristics such as renal or liver function, age, history of bleeding, and the use of other medications like antiplatelet agents or NSAIDs, must also be considered when deciding whether to stop anticoagulants before surgery (11). Restarting anticoagulants too soon can lead to postoperative bleeding, while delaying them too long can cause thromboembolism. In general, anticoagulants can be restarted 24–48 hours after surgery if bleeding is under control and the patient is stable (11).
References:
