
by Amin H. Karim MD
Here is a case of the Left Circumflex coronary artery arising from the right sinus of Valsalva. (Type I anomaly). This happens in 0.3-0.6 percent of cases. Patient was a 42 year old lady presenting with atypical chest pain. The anomaly is usually benign but can be associated with non atherosclerotic coronary artery disease and myocardial infarction.
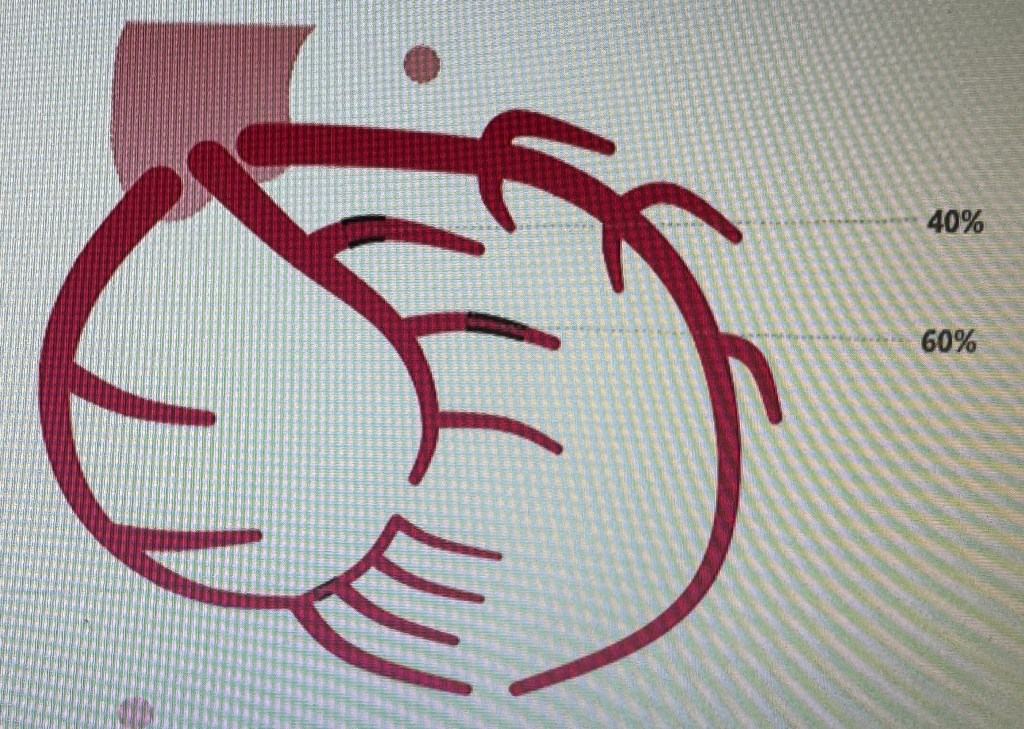
There is moderate occlusive disease in the branches of the left circumflex and the posterior descending coronary artery. It was decided to treat medically.
The anomaly brought to memory the pre-stent days of plain balloon angioplasty. We had a similar case in the 1980s presenting with unstable angina. Cath showed the anomalous origin and an ulcerated plaque in the body of the circumflex. We proceeded to do balloon angioplasty. Unfortunately, the artery dissected. We knew as trainee fellows that this was bad news. There were many measures which interventional cardiologists took to “tack up” the intimal dissection and restore the flow to the artery. Most common first attempt was to advance the same balloon back and try longer inflations as much as the patient could tolerate watching the ST Segments and the blood pressure and listening to the patient. If that did not work we tried larger balloon with low pressure inflation. In some cases it would make the dissection worse but worked sometimes. Some attendings would would try to find where the dissection started proximally and start dilating there. In any case, the procedure would go on for long. Late Dr. John Lewis would get suggest that this was all “inflammation of the artery” and would give ibuprofen to the patient. When this would not work and the artery would look more messed up he would say that “there is more trouble in the artery than in the middle of downtown Beirut” keeping in mind there was war going on in the Middle East at the time. In the meantime, the irate cardiologist who was to follow in the same room would be watching from the glass partition. And the good cardiovascular surgeons who graciously gave us “surgical backup” (mandatory in those days) would be waiting in the wings to see when we got tired to let them take the patient to the OR and operate….. 🙂 Those were the days….. (Amin H. Karim November 30 2013)
