
By Amin H. Karim MD
Parth Desai MD (Interventional Fellow)
CASE REPORT:
A 61 year old Caucasian female presented with sever chest pains for 3-4 hours.
EKG was obtained.
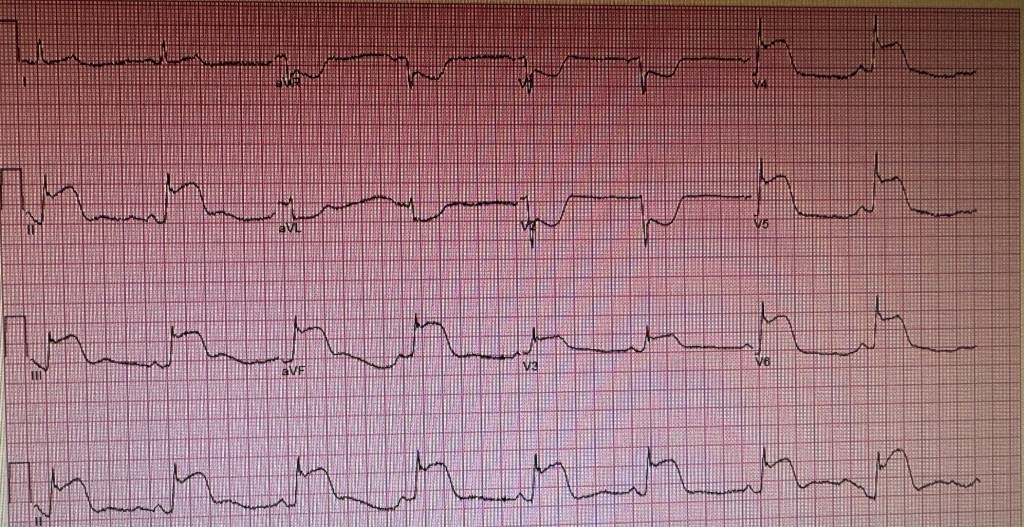
We put it through our panel to see if they could figure out the location of the culprit lesion in this STEMI patient. The answers ranged from a large dominant circumflex or RCA to a combined lesion in the LCX and LAD.
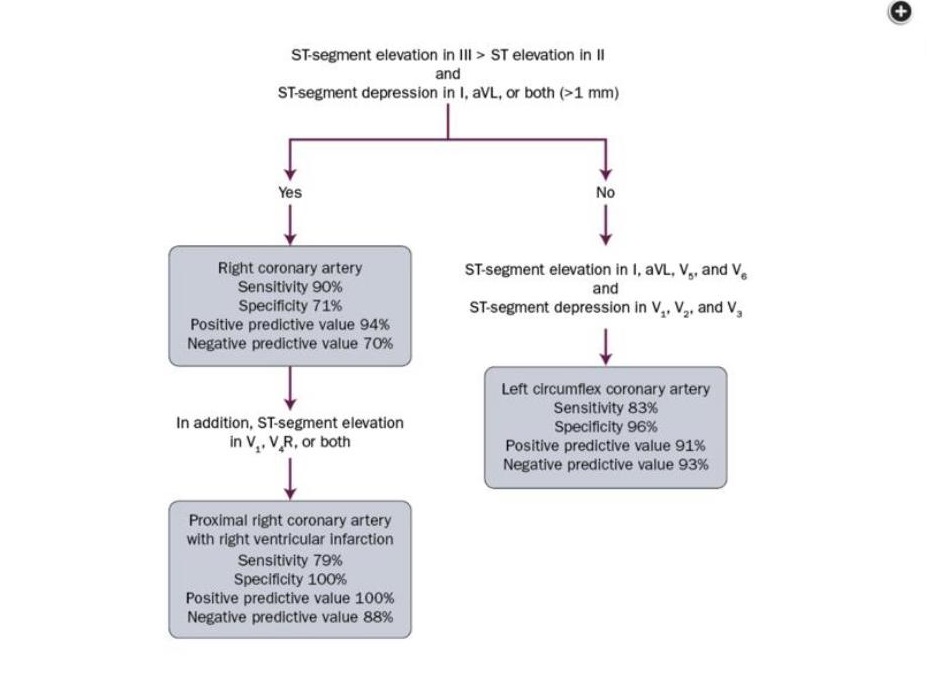
Take a moment and see if you can tell the location of the lesion. Perhaps you can use the chart that was went by Dr. Syed Fazal:
Cath showed the following:
We crossed the LCX lesion using a whisper wire, pre dilated it and placed a 3×18 mm Synergy DES with a satisfactory result.
So the question remains, why the extensive changes on the EKG when the lesion is localized and one would have expected changes in the inferior or inferior and lateral leads. Could the patient have a hypercoagulable state? malignancy?. There is no evidence of spontaneous dissection. Concomitant spasm in the LAD with the thrombus in the LCX is a possibility (reported by us in 1990’s and the two published articles are on this website). her troponins peaked at 8500. Echocardiogram showed wall motion abnormalities as follows:

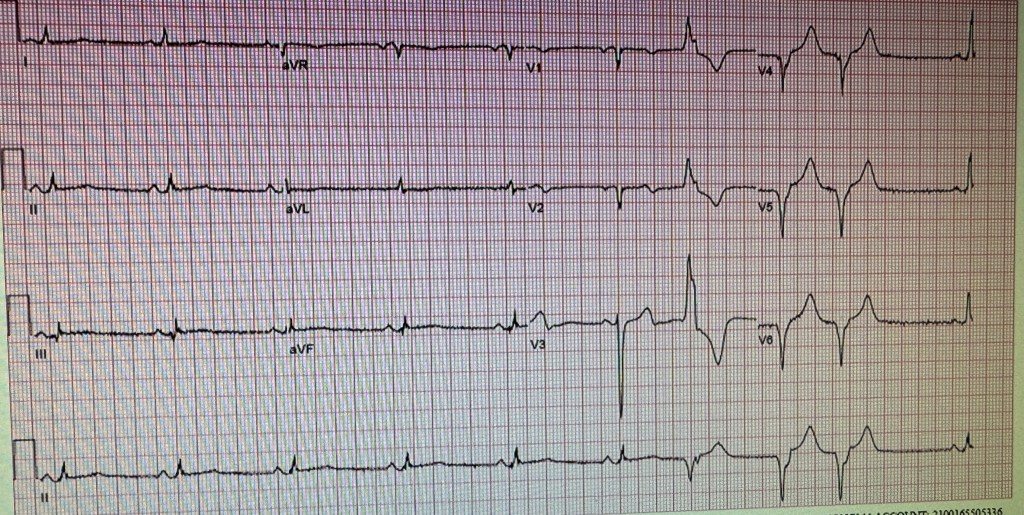
EKG done the next day. Patient did well clinically. The global ejection fraction was 45-49%.
Incidentally patient also took Adderal of and on for attention deficit disorder. There are reports that these drugs can increase the incidence of cardiovascular events.
INDEBTED TO COMMENTS ON THIS CASE BY:
Prof. Salman Arain
Dr. Syed Arman Raza
Dr. Farhan Katchi
Dr. Zubair Mohammad Syed
Dr. Syed Fazal
Dr. Usman Mustafa
