
By Dr. Salman Arain
McGovern Medical School, Houston, Texas.
February 10 2024
There are several ways to approach a CTO. The entire crossing process, whether antegrade or retrograde, starts with crossing the cap. Different techniques have been described. In my practice, I like to use contrast to modify and modulate the cap/plaque…
History. 68 year old man with LAD PCI 4 years ago. Presented with angina and found to have a new RCA lesion (which was stented) and this LAD CTO. The angina has resolved but the exertional dyspnea persists. The PET was very abnormal in the AW.
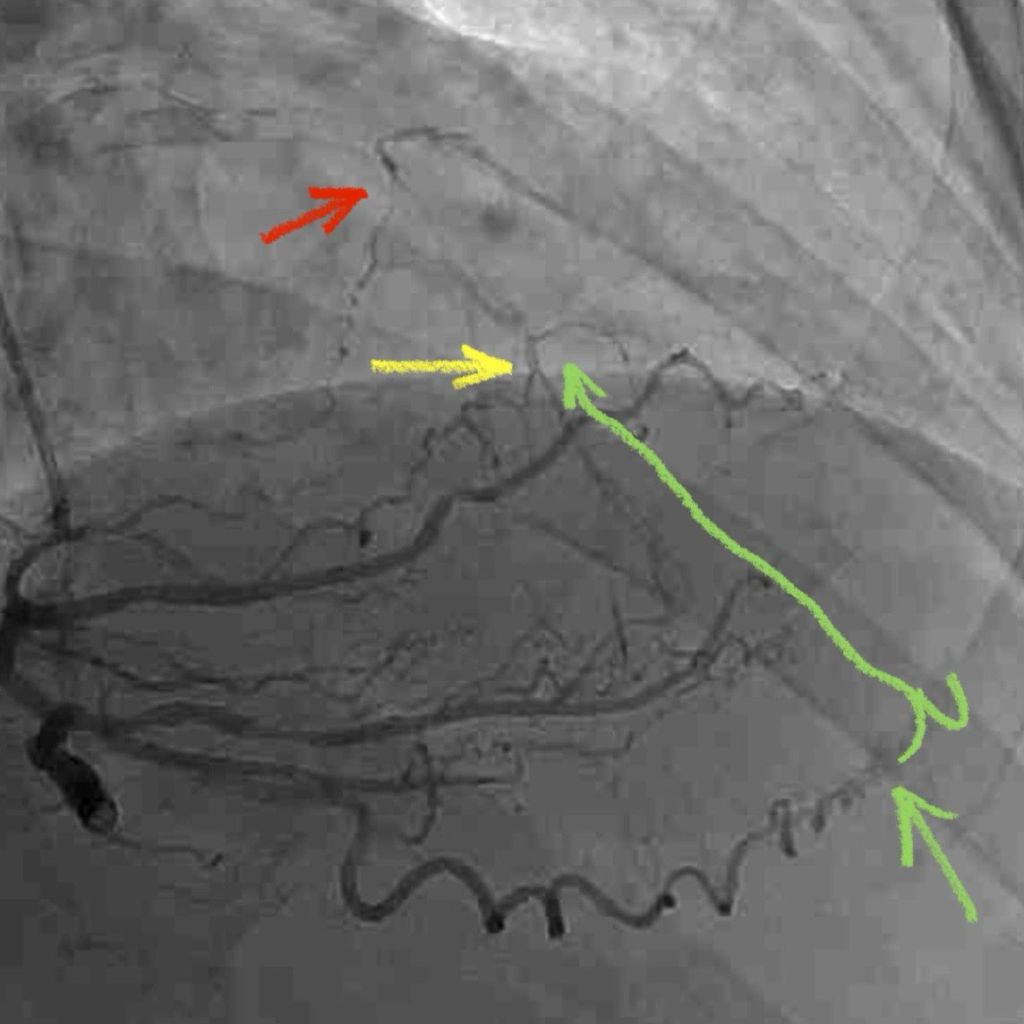
There are 3 sets of right to left collaterals. Not all are ‘usable’. The LAD fills in ‘stages’ which suggests disease in the native LAD beyond the CTO.
Plaque penetration was more challenging than expected. That is a Hornet 14 wire (14 gm penetration force at the tip!). As per our protocol, we stopped once the wire was a few mm distal to the hard cap. We then maneuvered our microcatheter (MC) in place.
Contrast modulation. 👆🏼Here is the intra-CTO contrast injection! Note the free passage of an tapered tip hydrophilic wire (Fielder XT).
Here is a distal tip injection. This is different than injecting into the occlusion. Transducing pressure allows is to confirm we are across before injecting. A softer tipped hydrophilic wire (Gladius Mongo) helped us track into the true LAD.
I like to perform IVUS before stenting to understand the nature of the CTO, the characteristics of the vessel wall, and the size of the lumen. This helps us choose the appropriate vessel preparation and stent therapy. Here our crossing is all intraluminal.
Here is the final run. We did multiple IVUS runs to size the LAD and optimize both the LAD and the D2. Note that all septals have been preserved! All in all a successful CTO which we completed in under an hour and a half.
