
Using Contrast To Cut The Gordian Knot! A Complicated CTO Intervention
By Dr. Salman Arain
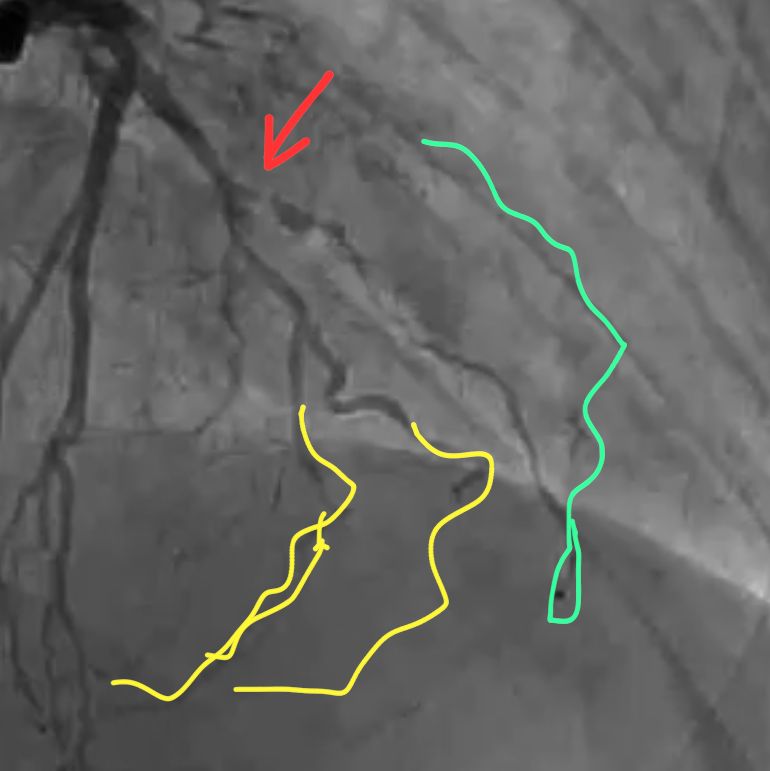
This is the complete angio. The patient is 57 years old with CCS 3 angina. He had bypass surgery 13 years ago. His EF is 35 to 40%.

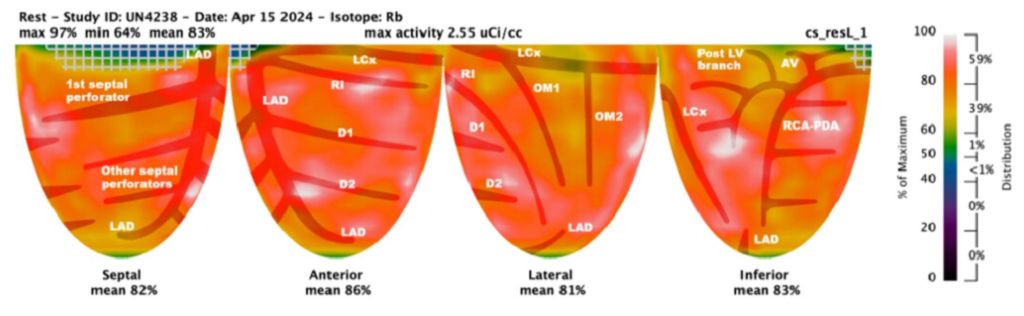
Viability Study
So, the question for our Cardio experts:
1) What do you recommend? PCI, re-do CABG, EECP or OMT alone?
2) If you choose PCI, which vessel would you go after first?
3) And what CTO strategy would you use? Retrograde PCI may or may not be the best answer here.
4) What do you know about the coronary sinus reducer, and would you consider that?
Tricky. The problem with the LCX is that the caps are all ambiguous and there are several bifurcations.
The LAD CTO is long but at least there is a well defined cap and a relatively straight course. Unfortunately the LAD septals supply the PDA which itself is occluded proximally and does not connect to the PLBs.
The RCA is the trickiest of all three. One thing to keep in mind is that the patient is post CABG – so any perforations would be more difficult to treat.
Ok, here is how it all played out. First a few thoughts about choosing the vessel to intervene upon.
The LAD has the most favorable anatomy but needs to be fixed least urgently. The proximal 1/3 is patent and the mid segment has a graft.
The LCX has an ambiguous cap and several branches that need to be rescued. It is important not only because of its own distribution, but because it is the best retrograde conduit to the RCA via the PLB.
RCA is the trickiest because it requires a combined antegrade and retrograde approach. Also, the PDA is occluded and is cut off from the large PLB system. So an occluded bifurcation somewhere!
Thus, we decided to go after the LCX – it was the one that would give us the greatest advantage in addressing the RCA.
Here are some dual injection angios to better show you the connections.
There are several ways to tackle a CTO – some antegrade and some retrograde. We have focused on and specialized in contrast modulation of plaque. This requires puncturing the proximal cap and then using micro injections of contrast. The technique is also called a modified Carlino injection after Mauro Carlino who described
Here is the setup for the LCX intervention by means of CAP (aka Carlino). Notice the ambiguous cap.

This is not the typical cloud. It is tubular which means we must be extra plaque
So we used a Gaia 2 to redirect our MC and repeat the contrast injection. Now we see the vessel architecture – as well as re-entry!
This is just the injection clip. The typical result is seen towards the LCX. There contrast mediated STAR into the OM2!
So we wired the LCX first, then treated the bifurcation, and used a dual lumen catheter to wire the OM2.
We used IVUS to confirm that we were not going to jail off the side branch with our stent. We used JSBT!
And here is the final angio. You can see that we are nicely set up for a retrograde intervention on the RCA in a few weeks.
And now you have the complete name for the case: Using Contrast To Cut The Gordian Knot! A Complicated CTO Intervention
Afterword. I think this case highlights how far coronary PCI has come – as a specialty. In my fellowship, this talk of dissecting and injecting contrast and going epicardial would have been blasphemous. And now it is routine in selected centers of course.
The upshot is that CABG is no longer the end of the road. The end of the road is the end of the road – and that is not in sight for coronary PCI!!!
Dr. Zaka Khan wrote: Regarding Coronary sinus reducer – This was original developed by Neovasc . A Canadian startup. There main two products for Cosira and Tiara. Cosira was designed for controlled occlusion of CS to improve symptoms of refractory Angina . It does improve at least 1 CCS class. Would work only in cases of refractory angina and evidence of reversible ischemia. It increases coronary microvasculature flow.
Tiara was supposed to be Transseptal Mitral valve replacement system without need for apical approach.
Company got into litigation with Edward’s and then few guys at UPEN. Material used for Tiara was manufactured by Boston Sci and hence they jumped into the mix. Cosira system was bought into by Shockwave medical.
Tiara is still somewhere and the fight goes on.
Many investors lost money because of legal battles. Would have been a big hit like TAVR .
Questions by Dr. Afaq Motiwala answered by Dr. Arain:
) Does the micro catheter injection into the cap create more extensive dissection (if you are extra plaque) and make it harder to get into true lumen? Yes and no. That is where we have honed our technique. It’s all a matter of understanding the contrast cloud.
2) How did the ivus help you with side branch? It helped confirm that I was in true lumen and that the side branch was not jailed behind plaque.
3) Where did you place your balloon for jsbt? Balloon from OM2 to top branch and stent in the main body of the OM2
4)The small branch you preserved with a wire, does it have some contained hematoma? Any need to tamponade it or it’s inconsequential? It does, but the flow was good without a dissection in multiple views. So OK to follow clinically. These are very small branches.
.
It was important to preserve the OM2 trifurcation. You can see the size of it in the cranial view. The top branch fills OM1 and the bottom two supply the PLB. I plan to fix both eventually.
Dr. Amin H. Karim wrote: The cath diagram took me back to pre-EMR days when we routinely made these after watching the cine on Trajano. They were very reflective of the coronary anatomy as well as recording one’s personal notes. 30 years later when we look at these in the patient’s chart it gives a good idea of the pre-intervention anatomy. Computer diagrams are no match and I feel sorry for your younger colleagues when they pull their patient records decades later, they will be looking at a computer cartoon that is a far cry from the real anatomy. Both Michael DeBakey and Denton Cooley gave a lot of importance to the cath diagram on patients referred for surgery and both would hang them on the old x-ray box in the OR as a reference! Dr. DeBakey would meticulously put his pencil notes on the diagram and file them on each patient. He would also draw the grafts on another copy and send them to the referral cardiologist. He would pull the file out when patient came in years later for redo
