By Dr. Arnav Kumar MD, MSCR Interventional Cardiologist HCA Medical Center Hospital Houston, Texas
87 year old extremely pleasant, active woman was sent to us for complex LM PCI . She has distal left main 70% disease, ostial LAD 70% disease, calcific 90% disease of the proximal high Obtuse marginal artery and 99% Proximal LCX disease.
The left main itself is very long and anomalous. We anticipated challenge in delivering equipments across the retrofelxed LCX. Additionally, she has distal RCA disease . She was felt to be too high risk for CABG due to advanced age We were able to cross the ostial LAD – lesion using a sion blue wire. We were able to cross the high OM lesion using a minamo wire.
Crossing the 99% very calcified proximal left circumflex lesion proved challenging. However, we were able to cross it using Fielder XT.
Retroflexed LCX, anomalous long LM have high risk of stent dislodgment left main dissection and wire dislodgement.
The plan was to do double cush- however, no stent would go across the LCX lesion. We first pre dilated LM, LAD, LCX, ON lesions. We did encounter challenges in delivering balloons into LCX. After Predilation, we placed a stent in the OM and crushed it with a ballon placed in LM-LCX. However we faced extreme difficulty in placing stent in the LCX-LM. Finally, we had to take out both the OM and the LAD wire and were successful in delivering the stent across the LXC lesion using guideliner support (advancing the guideliner in to the LCX). After deploying the stent In the LM-LCX, we post dilated with an NC balloon.
We quickly crossed back into the the LAD – ie switched to a coullote technique..
Final angiograms demonstrated excellent stent expansion, no edge dissection and no geographic miss.
Impella was taken out at the end of the procedure and LFA was perclosed. Patient underwent PCI of RCA two days later and discharged home In great spirits
Extremely retroflexed LCX – showing that all stents started prolapsing- unable to deliver; Had to sacrifice LAD, OM wires to advance a guideliner into the LCX… and hence was able to place a stent into the LCX-LM. However this meant that we had to change to coullote technique; Placed a stent in the LAD – LM
Then simultaneous kissing balloon inflation of the LAD-LM-LCX
By Paulina Maldonado Universidad De Durango, Chihuahua, Mexico Houston, Texas. Amin H. Karim MD Baylor College of Medicine and Methodist Institute of Academic Medicine, Houston, Texas
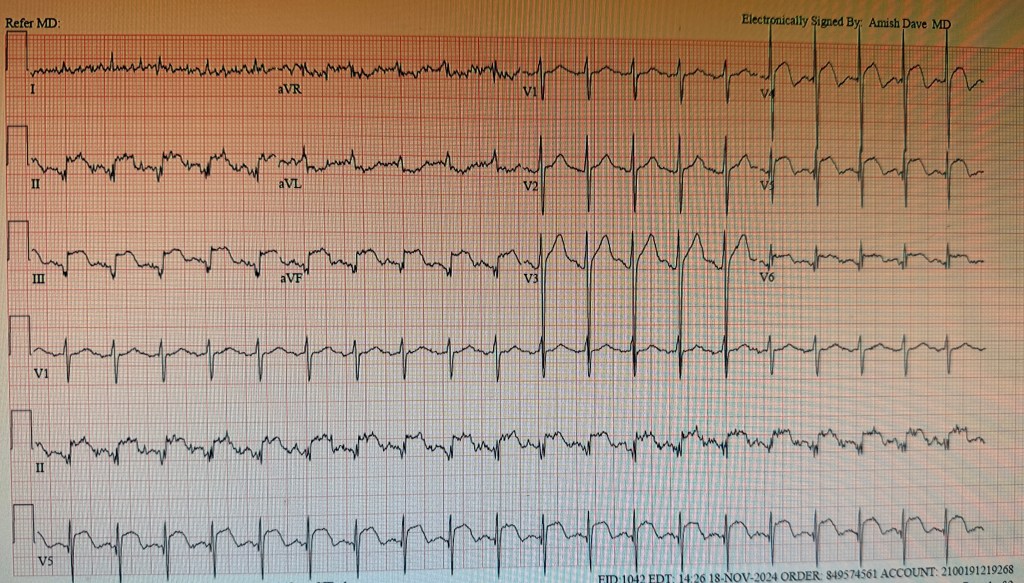
A 65 year old patient presented, disabled from old cerebro vascular accident causing flaccid left sided hemiplegia with contractures, admitted to hospital for change of mental status; he developed hypotension; EKG showed ST elevation in II, III and aVF as well as V3V4V5 diagnostic of inferior wall myocardial infarction with lateral extension.
He was rushed to the cath lab where cardiac catheterization showed what looked like “normal coronary arteries”.
His high sensitivity peaked at 1200. He was treated with intravenous heparin and beta blockers; he remained hemodynamically stable and was discharged.
Myocardial Infarction with nonobstructive coronary atherosclerosis
Although the occurrence was initially reported about 80 years ago a very small number of patients are found to have MINOCA.
The term MINOCA is reserved for patients with elevated troponin associated with myocardial ischemia at presentation and should not include disorders with non ischemic elevated troponin.
It is important to mention and reiterate that MINOCA should not be considered a final diagnosis but rather a working one that requires further testing.
Epidemiology
The incidence of MINOCA varied from 1% to 15% and roughly 6% of all Acute Myocardial Infarction cases.
Younger (18-55)
Female
lower prevalence of hyperlipidemia
⅓ presented with ST segment elevation of myocardial infarction
Pathogenesis:
MINOCA is heterogenous and can be divided into coronary, cardiac and extra cardiac causes. Ischemia happens during a temporary suspension of blood flow to the myocardium and it takes place in the epicardial arteries or the microvasculature.
Coronary
Cardiac
Extra cardiac
plaque rupture or erosion
Myocarditis
stroke
coronary spasm
Takotsubo syndrome
pulmonary embolism
spontaneous coronary artery dissection
cardiomyopathies
sepsis
coronary embolization
cardiac trauma
renal failure
coronary microvascular disorders
tachyarrhythmias
hypoxemia
Risk factors:
Associated with Long term major adverse cardiovascular events after MINOCA including ST segment elevation on a presenting Electrocardiogram
older age
reduced left ventricular ejection fraction
diabetes mellitus
hypertension
tobacco use
prior Myocardial infarction
Stroke
peripheral artery disease
chronic obstructive pulmonary disease
chronic kidney disease
lower total cholesterol
Peak troponin
Depression at the time of MINOCA
Signs and Symptoms:
Chest pain/chest pressure / chest heaviness
Nausea
jaw, neck or upper back pain
pain or pressure in the lower chest or upper abdomen
shortness of breath
fainting
indigestion
fatigue
Diagnostics:
Requires a comprehensive diagnostic workup. Is the first line diagnostic tool to detect non obstructive epicardial coronary arteries (less than 50% stenosis) in the setting of an Myocardial Infarction.
Imagining modalities are vital in diagnosing and identifying the underlying mechanisms of MINOCA.
Coronary intravascular imaging
With Intravascular Ultrasound 40% cases and Optical Coherence Tomography 50% cases is essential to diagnose plaque disruption.
It should be performed at the time of coronary angiography for Acute Myocardial Infarction in all 3 major epicardial arteries.
Cardiac Imaging
Transthoracic echocardiography used in the assessment of cardiac function after a MINOCA. It can be used in the diagnosis of Takotsubo cardiomyopathy and non ischemic cardiomyopathy specifically to demonstrate recovery of left ventricular function.
Transesophageal echocardiography can be used when coronary embolism is suspected.
Cardiac Magnetic Resonance Imagining (CMRI) provides a diagnosis in 74-87% of all MINOCA patients.
Subendocardial (or transmural) pattern of myocardial edema, inflammation or fibrosis is suggested of ischemic Myocardial Infarction.
Epicardial pattern is suggestive of non ischemic Myocardial Infarction.
Echocardiogram can be used to diagnose Takotsubo cardiomyopathy and non ischemic cardiomyopathy, but CMRI can only be used to detect myocarditis.
Myocardial perfusion quantification with adenosine or regadenoson can be used to diagnose coronary microvascular dysfunction non invasively.
The timing to perform a CMRI is important; it should be completed as close to the acute myocardial infarction as possible. CMRI carries not only diagnostic value but prognostic value as well.
Multimodality approach
OCT and CMRI together resulted in a diagnosis in 85% of the cases whereas Optical Coherence Tomography alone was only 46% and Cardiac Magnetic Resonance Imagining 74%.
Treatment
It should me customized to the underlying diagnosis:
Meds
Underlying diagnosis
Aspirin and High intensity statins
Plaque disruption
dual antiplatelet therapy by adding ticagrelor for less than 1 month
Plaque disruption not undergoing stenting
Beta blocker and renin angiotensin system inhibitors
left ventricular dysfunction
Long acting calcium channel antagonist (dihydropyridine and nondihydropyridine)
MINOCA patients secondary to epicardial coronary vasospasm
nitrates can be added to calcium channel antagonists
refractory variant angina
antithrombotic agents
coronary embolism or thrombosis
targeted therapies
underlying thrombophilia
conservative management (avoiding increased risk of complications with intervention)
spontaneous coronary artery dissection
Percutaneous coronary intervention
STEMI, cardiogenic shock, ongoing ischemia
aspirin, beta blocker, statin and renin angiotensin system
spontaneous coronary artery dissection (should be assessed based on individual risk factors
antianginal treatment with b blockers, calcium, channel antagonists and ranolazine
Chest pain
MINOCA mimickers
Heart failure
mechanical circulatory support
progressive circulatory failure
resolves in most patients within 2-4 weeks
Myocarditis, but if they develop arrhythmia and persistent cardiac dysfunction medical therapy should be administered.
antivirals and immunosuppressives
underlying etiologies
Prognosis:
Short and long term mortality
At 1 year follow up, MINOCA mortality is 2 to 5%.
Among individuals 65 and older the risk of adverse outcomes is higher 12%
Possible Reinfarction
only occurs in 1.3 to 2.6% of patients at 1 year and 7.1% at 4 years.
Quality of life
Identified factors that increase the risk of Major advance cardiac event:
older age
hypertension
smoking
reduced ejection fraction
chronic obstructive pulmonary disease
elevated creatinine
cancer
elevated CRP
Requires further investigation that may require longer hospitalizations. It is commonly found that Myocardial Infarctions is missed in women due to non classic presentations such as shortness of breath, dizziness, nausea or unusual fatigue. Patients with MINOCA do present with recurrent chest pains without myocardial infarction.
Literature Cited:
Tamis‐Holland, J. E., & Jneid, H. (2018). Myocardial Infarction With Nonobstructive Coronary Arteries (MINOCA): It ‘s Time to Face Reality! Journal Of The American Heart Association, 7(13). https://doi.org/10.1161/jaha.118.009635
Takahashi, J., Onuma, S., Hao, K., Godo, S., Shiroto, T., & Yasuda, S. (2023). Pathophysiology and diagnostic pathway of myocardial infarction with non-obstructive coronary arteries. Journal Of Cardiology, 83(1), 17-24. https://doi.org/10.1016/j.jjcc.2023.07.014
Yildiz, M., Ashokprabhu, N., Shewale, A., Pico, M., Henry, T. D., Quesada, O. (s. f.). Myocardial infarction with non-obstructive coronary arteries (MINOCA). Frontiers In Cardiovascular Medicine, 9. https://doi.org/10.3389/fcvm.2022.1032436
De Oliveira, L. L. H., Correia, V. M., Nicz, P. F. G., Soares, P. R., & Scudeler, T. L. (s. f.). MINOCA: One size fits all? Probably Not—A review of etiology, investigation, and treatment. Journal Of Clinical Medicine, 11(19), 5497. https://doi.org/10.3390/jcm11195497
Talking JSKBT ( jailed semi inflated kissing balloon technique ) We did multiple JSKBTs here. Zameer our Pakistani fellow made these images.
Patient had CP/ NSTEMI in a decent sized town 100 miles away. Which has good sized hospital and interventional cardiologist’s and PCIs / primary etc are done. No CABG onsite. Cardiologist did angio for intervention purposes. Saw the anatomy Calcified distal left main, Ostial/ prox / mid LAD, 90% tight ramus, 90% bifurcation LCX/OM1 and CTO RCA. EF 30% with severe MR ( so even poorer forward flow / and overestimation of the LV function due to MR).
Referred to our surgeon. He said he can ! But very high risk. ( calcified aorta not. Great candidate to put on heart lung bypass / previous EVAR, Poor LV function, ) so referred to one of our colleagues – who said very high risk PCI. Referred back to surgery. Nothing happened. Meanwhile patient having symptoms. So the primary interventional cardiologist from the other city called us. Was going to need 3 to 4 wires with multiple balloons at a time. So needed an 8 French guide so did do single access Impella. Also deliberately took a short JL 3.5 guide ( which obviously has low support ) so we can sit outside this shortish left main and work
LAD was quite retroflex so you can appreciate flipping of hydrophilic coated wire with >120 bend with microcatheter assistance. Later changed to wiggle wire; So onwards LAD was started. Calcified, retroflex and quite some tortuous so IVUS was done after first run of 2.5 pre-dil; Still there was IVUS malfunction in mid autorun so predilated with 3.0 balloon and ReIVUS Heavy more than 270 degrees calcium is there; Further vessel preparation was done with 3.0 IVL all the way upto LMS
This is tight LCX and tight OM1. Kissing balloon inflations and then stent in LCX and JSKBT is OM. Notice 4 wires in there. Pretty good result. OM Latium looks really good. IVUD of LCX stent good. Did POT of the proximal LCX with NC balloon; This is the long 3.0 x 48 synergy xl. Extending from mid LAD to left main and have 3.0 x 15 balloons as JSKBTs in Intermediate and LCX
Couldn’t get the IVUS to distal edge to see if it is dissection or spasm. These new Hi Def boston IVUS shafts are flimsy and you push them and they get bent. Used three different catheters during this long intervention. Cuz it would get stuck in calcium and then either stop working or the shaft get bent. So images look like distal edge dissection. Placed a 2.5 mm shirt stent. Looked good after wards
IVUS from LAD stent back to left main. Had also done a 4.5 x 6 mm short NC balloon POT for left main. ( size mismatch between left main and LAD)
Of course without Impella. Wouldn’t have been able to do these. With occluded RCA and EF 30% with severe MR. I was getting flat line pressures with IVL and Thenleft main stenting with JSKBTs