WIDOW MAKER LESION I cath a patient with chest pain today as an emergency. The patient asked: “What did you find, doc?” I said ” I found a narrowing in the big artery that goes to the front of your heart”. He said: “You mean the widow maker lesion” I said: “No Sir, it used to be called the widow maker lesion. Now it called the New Husband Maker Lesion” It made him laugh.
SICK SINUS SYNDROME: Today a elderly cardiac patient asked me if the metoprolol he is taking will affect his sick sinus syndrome. I was a bit surprised. I said it certainly can do that and slow the heart rate. He said ” Doc, then I should not be on it!” “But” I said. “How do you know you have sick sinus syndrome?” He remarked: ” I have had sinuses for a long time and I read on the internet that metaprolol should not be taken if you have sick sinuses” (Amin H. Karim MD)
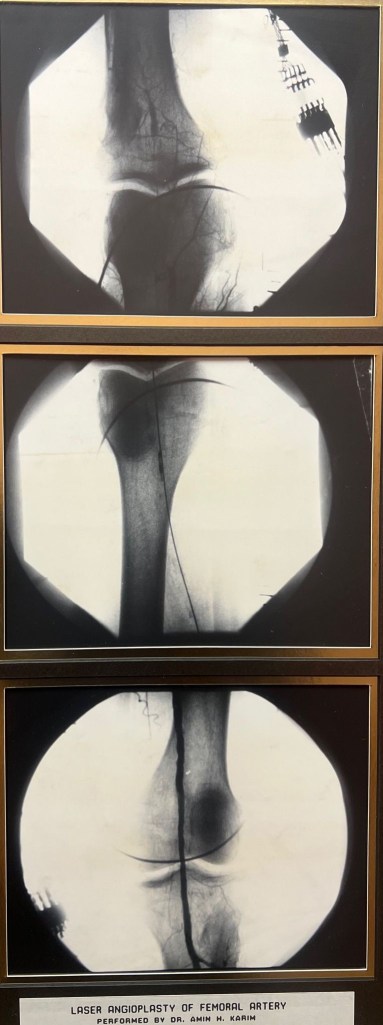
Interventional friends; here is a piece of history. The year is 1989 ( 34 years ago). Excimer ( short for excited dimer) was approved for peripherals and later coronary use; we, in Houston, were one of the first to try it out after attending a laser safety course. Above is an angioplasty on a CTO of femoral artery. The probe went in ( without wire) like a “knife through butter” followed by wire and balloon ( stents had not been invented yet) of course as expected there was thermal damage to intima and reactive fibrosis and Re stenosis. But did have impact on patient psyche of having “ cutting edge” procedure ( no pun intended).
The author can be reached at globelinker@gmail.com
That’s Norman Shumway, the first to perform heart transplant in USA in 1968, after Christian Bernard did the first in the world in 1967. ( I had just graduated from school!) . Unfortunately never met Dr. Shumway, although he may have come to Texas Heart Institute and known Howard Frazier who was into heart transplants in Houston. Shumway died in 2006 of lung cancer. Amazingly, two other legends at Houston Methodist Stanley Crawford, pioneer of aortic aneurysm surgery, and Jimmy Howell, both smokers and both died of lung cancer!. May they all rest in Peace. They gave a lot to humanity. They lived in times when doctors advertised smoking for asthma!
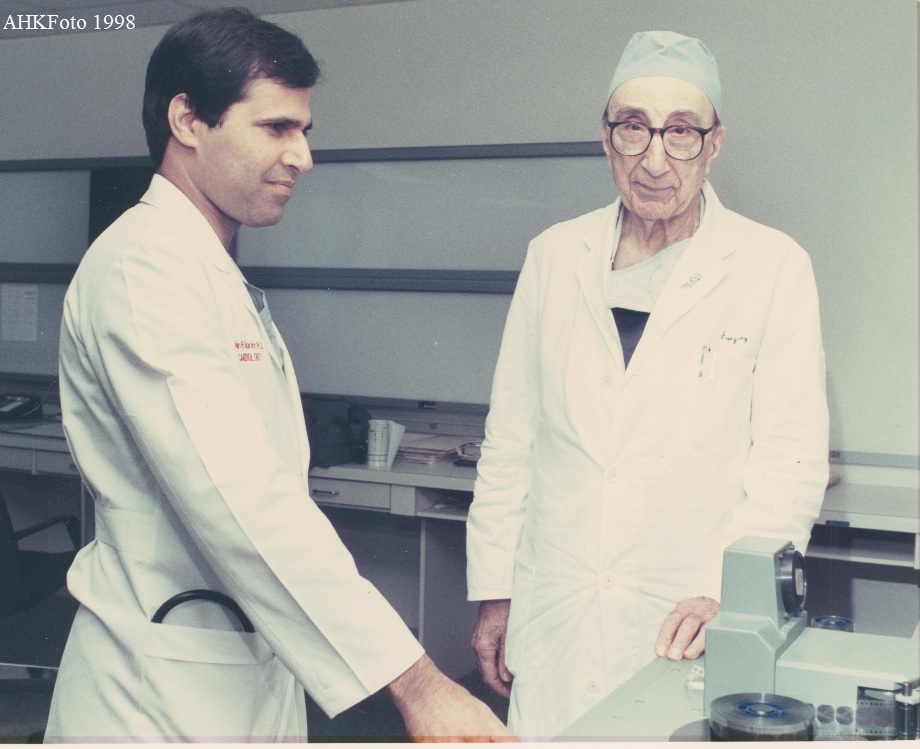
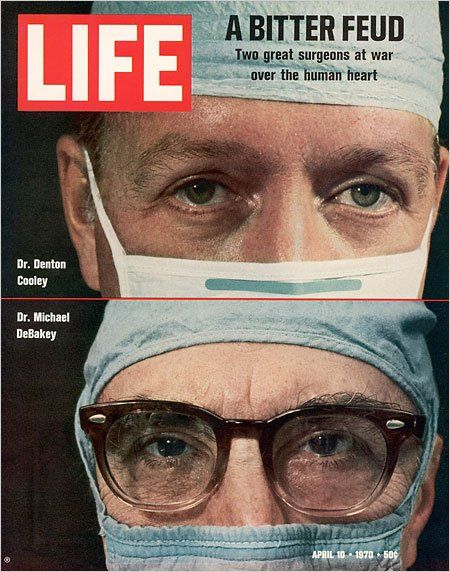
ABOUT Dr. DEBAKEY
It is said as a kid DeBakey who grew up in New Orleans went to the school library and asked the librarian if he could borrow the Encyclopedia Brittanica; the librarian of course told him he cannot since it is a reference. His dad bought a set for him and he read all the volumes cover to cover.
MEDs preferred cardiologist was Dr. Mohammed Attar, a solo like me; he probably liked him because Attar is very good and meticulous and also because his roots are in Syria and Lebanon like Dr DeBakey. Attar and I covered each other for more than 20 years. MED daily rounds would start exactly at 3 pm. He would be walking VIP the stairs with his entourage of Dr Attar, fellows residents behind. One nurse said you guys look like a hen followed by chicken. 🙂 when Attar was out of town I would have to be ready by 3 and know all his patients like an intern! But he was always nice as long as you knew the patients.
Dr. DeBakey had his office on the 9th floor of Fondren Building in Methodist. He had the privilege of holding the fireman’s key to the elevator. When he got in he would use the key and press 9 which means elevator goes straight to 9. One was supposed to leave the elevator regardless and he would ride up. May he rest in Peace.
Some good things about MED ( initials for Michael E. DeBakey) he did open hearts by thousands. Kept a file on each patient. If we Cath his patients later we would have to send a diagram to him. He would carefully record the findings comparing with the ones before and after surgery and write pencil notes. His office was inside the hospital; he stayed on full time faculty of Baylor till the end and never did private practice. Passed away in 2008 at age 99.
Late Denton Cooley certainly was the more friendly of the two. He held cardiologists close to his heart inviting them to his ranch every year ( Cool Acres Ranch in Rosenberg) for BBQ. He would play softball with the kids he had 5 daughters ( some were surgeons). Cardiologist Virendra Mathur made him famous in India and many came to him including Kishore Kumar, Madam Noor Jehan and others. When General Habibullah ( Gen Ayub Khan’s samdee) who was Mathur’s patient when he found out there was a Pakistani cardiologist next door in Methodist he switched over and he remained my patient till the end; same happened with some others from Pakistan. Later Cooley did not get into newer techniques like mini cab calling them gimmicks.
Certainly Naeem as time permits; have seen and worked with both of them over the years and of course heard a lot of Doctors Lounge Talk. I was one if the blokes who was on good terms with both these “ rivals” in two neighboring hospitals. Late Oro dental surgeon Oscar Moldonado and Dr. George Noon would similarly claim!
I will try to keep what I write free of what can even remotely be construed as gossip or back biting (the latter strictly not allowed in Islam). Will write what I saw or others who I trust recounted. Of course, being busy and running to different hospitals to make a living, there was no time to record numbers and stats. etc ( not easily revealed by hospitals anyway). Blogs better than books since they can be updated and read by all for free. History aside, maybe other interventionists will take a hint and start their own blogs and record their interesting cases and how they were treated ( I see some remarkable cases on WhatsApp groups). Later new fellows can benefit from it. WhatsApp and FaceBook messages are fleeting. YouTube can also be used similarly by creating your own channel. Just have to make sure patient ID remains hidden (we know the rules) Youtube is universal and residents all over the globe can benefit. This is all informal, ongoing and individually powered and costs nothing.
A 85 year old patient on hemodialysis, presented with acute coronary syndrome. Cath showed a totally occluded RCA. This is just a straight forward case being posted initially to test the website and ease of uploading videos.
Here is the left coronary showing a tight proximal LAD but not a culprit lesion.
View of left coronary showing a tihth proximal LAD lesion but not the culprit.
Anohter left coronary view showing collaterals to the RCA.
A large occluded RCA in the proximal portion with a possible clot.
RCA double sired with a High Torque Floppy wire and a Sion Black wire.
Lesion predilated and stent with a Synergy DES 4.5 x 28 mm stent and post dilated with a 5.0 x 15 non compliant baloon at nominal pressues. TIMI 3 flow achieved. Intracoronary nitroglycerin and intracoronary nitroprusside used. Patient remained stable throughout. Stent placement in the LAD is planned in 3 days.
Prof. Michael E. DeBakey is nothing short of a legend of Medicine. He was the Head of Department of Surgery at the Baylor College of Medicine, Houston, Texas.
This write up is not meant to write his bio. He already has books written on him. These are just quiet observations of someone who worked at the Houston Methodist Hospital from 1984 to date and saw and worked with the Professor as a non surgeon and for a limited time. Prof. DeBakey rounded Monday to Friday starting at 4 PM. He carried a patient load of roudndly 100-120 patients at a time. He was very meticulous and expected to know details on each of his patient. The resident responsible for the patients had to be on his/her feet and expected to know progress, labs, vital signs and report to the Professor. Dr. DeBakey expected all the consultants, some Chiefs of their own departments to accompany him on the rounds so that quick decisions could be made. This included the Cardiologist (sometimes more than one) the Internist, the Nephrologist, Infectious Disease Specialist, Pulmonologist and the like. The attrition rate of residents was about 20% either resigning due to stress and could not take it any more or being fired on the spot.
FONDREN ICU RESIDENT: The Cardiovascular ICU was the location for this famed rotation which all CV residents had to undertake and was one test of nerves and patience. Professor likely used this as The Test to see who could survive his training and come out a trained surgeon. First it was straight 3 months ( as related to me by Dr. Phillipe, Urologist) and later it was changed to 60 days done twice. (related to me by Dr. Hazim Safi, CV Surgeon) During this rotation, the resident LIVED in the ICU and was not allowed to leave till the rotation ended. He/she slept in the isolation room ( no attached bathroom, just a sink) and was on call 24/7. His job was to round on each and every patient in the ICU and write notes, and fill out the detailed labs on each patient to present to the Professor during rounds. In the early days there was a RED LINE which could not be crossed by the resident to go out. (more about this later). Actually less residents were fired from this rotation than on the other rotations, likely because by the time they came to this rotation they had already weathered the “storm”.
PROFESSOR DEBAKEY’S RED LINE:
A red line similar to this one once was at the entrance to the Fondren ICU at the Methodist Hospital, Houston, Texas. It represented the line that could not be crossed by the surgical resident doing his three month rotation in the Cardiovascular Intensive Care Unit. Once the resident entered the Unit he stayed there for the next 3 months, sleeping in a room, working, rounding, writing notes, doing procedures, managing ventilators, admitting and discharging patients, accompanying Prof. DeBakey on rounds once or twice or more daily. There was no timing of rounds which could start and end when all the patients had been seen. Resident ate, drank, prayed, showered, shaved and slept when he could in the Unit. He could see his family once in a while through a small window. One thing he could not do till the last day of his rotation is to cross the red line. For if he did, it would mean an end to his surgical residency and his career. He would be dismissed from the Surgical program and from the Hospital. The following true incident was quoted by a surgeon (who is now a urologist) who actually did this rotation in 1960’s.There was a Philipino resident in the group. He had done 10 weeks of the rotation with 2 weeks more to go.He was excited and out of sheer fun he went near the red line and actually crossed it and bragged to the nearby patient liaison secretary that he had only two more weeks to go and then he would be free. Alas, his excitement was not to last long. The secretary promptly picked up the old black dialer phone and called Dr. DeBakey’s secretary and told her what she had noticed. Next morning at rounds, Dr. DeBakey singled out the resident, held him by the nape of his neck, dragged him to the entrance of the ICU and physically kicked him out of the Unit. The resident was expelled from the program. The reader can make his/her own decision regarding this incident. Was it his strict discipline that he himself practiced and he expected from his students for him to take this drastic action? Was it cruelty? Of course in this day and age this type of authoritarian practice would not be possible without inviting a lawsuit for assault. In fact might be criminal. You decide…..
👆🏼This is the case that almost got away. 58 year old man with a failed attempt by the referring MD. He has severe ischemia in the inferolateral region. He does not have LAD or left main disease, so not an upfront CABG candidate.
Tortuous RCA
Tortuous RCA
Here is the attempted intervention. The operator is experienced but does not do CTOs. He used an OTW balloon and some workhorse wires. He stopped because he was unable to cross and the patient started complaining of angina.
But before I do, let me just lay out some initial considerations:
Guide support
Crossing the tortuosity (or tortuosities!)
Prevention of spasm +/- accordion effect
Lesion prep – given the nodular calcium appearance.
I felt that a soft tipped hydrophilic wire was essential to start. Also, up front guide extension…
We used a Luge wire and a 6 Fr GuideLiner. Turns out, that this was the easiest part of the entire procedure. 😳 more to follow 👆🏼This is BAT. Balloon aided tracking. Very helpful for advancing guide extenders over long distances, when the path is relatively open. There is a 2 mm balloon, partially extending out of the GL tip. It is inflated to 4 atm. Both balloon and GL are advanced together. This is not my attempt. But my commentary is that the operator has good support but his choice of a microcatheter (MC) could have been better. Braided MCs perform better than OTW balloons and unbraided MCs. Also, the wire should ideally be a highly torquable wire with an appropriate tip. Most workhorse wires don’t have adequate support and/or the appropriate tip – hydrophilic tapered would be ideal.
This is our first attempt – we used multiple wires and tip shapes. Fielder XT, Sion Black, Fighter, and Gladius Mongo.You can see that I am using the Luge as a marker wire. I also have a dual lumen catheter so that the wires don’t interact (with the bonus advantage of support).
Anyway, in the interest of time and not to bore the audience with the drawn out style (which is how I teach!), we decided to take another hi-res view of the lesion. Turns out it is very complex because it comes off in a retroflexed manner, there plaque proximal to it which deflects the MC, and there is a hinge point which makes the lesion even tighter in systole!!! I have deliberately slowed it down here. So, last question. What do you do here? How to solve this twist in the tail?!
What we ended up doing (with luck as much as intention) is creating a ‘biplanar curve’ aka a spiral tip. It bent both downwards and to the side. This allowed us to ‘cork screw’ the wire (Mongo) into the PDA.
But, to put it in perspective, what looks like an obvious solution (now) took years of doing complex cases to achieve. And hundreds if not thousands of cases
Final thoughts. There are three ways to use a balloon to advance a GL.
Anchoring. Best for short distances with few bends. You can do it repeatedly as you go down the vessel.
Inch worming. This is where you deflate the balloon and advance the GL over it. Best for heavily calcified arteries and/or tracking within stents.
BAT. Best for arteries with extreme tortuosity, which are otherwise patent proximately. Or to go down open grafts.
Thank you but we tried all combinations I could think of. With all types of wire tips. Even a Carlino to make a channel and a knuckle. Nothing worked – primarily because the lesion is foreshortened in our initial working view and because the ‘hinge’ at the PDA origin changes the orientation of the opening with every heart beat. A dynamic stenosis! BTW, the wires we used included a Fielder XT, Fighter, Mongo, Sion Black, and a Gaia 2. The bi-planar tip is on the Mongo. And not with the usual curve added to the pre-shaped tip. Only after we gave it a sideways second curve. You can see it unfold a bit, before we were able to advance it across the stenosis.
Prof. Salman Arain
Permission to reproduce above obtained from Dr. Salman Arain on Nov 27 2023
North Pole is a small Alaskan city, near Fairbanks. It’s known for its year-round Christmas decorations, including candy cane–striped street lights. Santa Claus House is a Christmas store with walls covered in children’s letters to Santa and a huge Santa statue outside. Streets have names like Kris Kringle Drive and Mistletoe Lane;
It has a population of about 2300 people who are kind enough to volunteer for parents to send them gifts for children and they in turn mail it back to them via their post office so that they are stamped by the name “North Pole Post Office”.
Now, what has this to do with a Cardiology forum. I will tell you a little story with some history to it.
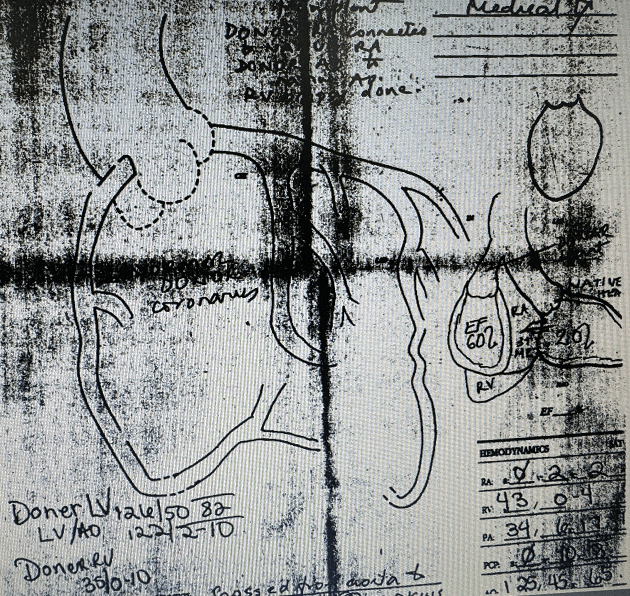
In late 1990s a 65 year old male patient from North Pole Alaska came to me with a complaint of shortness of breath. We found that he had end stage low EF congestive cardiac failure and after the usual workup enlisted him for heart transplant. He was lucky to get one and Dr. Howard Frazier ( who to this day has done the most heart transplants on the Planet) performed a rather atypical heart transplant on him. Instead of removing the entire front part of the recipient heart and suturing the donor heart over it, he did what was called ” a piggy back transplant” in which he left the native heart alone and connected the donor heart to the aorta and the RA/RV , thus creating a sort of ” Left ventricular Assist Device”. I am not sure what the exact reason for this experiment was but apparently he knew what he was doing The patient did well and went home and continued to improve for several months off this piggy back heart. He came back from Alaska and I did a cardiac cath on him as was the protocol along with an endomyocardial biopsy of the donor heart to check for rejection. I got the most strange experience of looking for two sets of coronaries and two left ventriculograms in the same person. The native coronaries were diseased but the donor coronaries were normal angiographically.
The patient continued to do well and became quite functional and tolerated his anti rejection regimen. One day, in 1999, he noticed a growth on his year and consulted his primary care doctor in Alaska who told him not to worry about it. Tragically, it turned out to be a melanoma that quickly spread to his brain and proved fatal. No wonder, to this day I still have his extended family and friends come to Houston for treatment as they do not trust the doctors there.
There are many websites, videos and blogs disseminating medical knowledge for learners, be it medical students, residents, fellows and practitioners across the Globe. GlobeMedic will do it a little differently. It will attempt to impart knowledge based on the experience of practicing physicians and surgeons and other professionals, in an informal manner. Not all patient encounters, thoughtful diagnostic workups of patient problems, innovative and skillful procedures and surgeries make it to published case reports. This website will allow the busy practitioner to share his/her experience and procedure details for others to know about.
It is hoped that these informal blogs, demonstrations and discussions will help followers learn a thing or two and either apply in their practice or use the knowledge to answer questions posed in certification exams.
What we do not purport to do: We do not issue Continuing Medical Education Certificates. We do not have any financial gain. This effort is entirely voluntary and in the spirit of sharing knowledge and knowhow for the ultimate benefit of ailing humanity wherever they may be.
HERE ARE SOME GUIDELINES FOR POSTING: These will be modified from time to time as more faculty is added and we learn from them.
Anyone can submit interesting cases, (with and without photos or videos) discussions, comments.
All content should be original and not been copied from other website or publication, unless you were the author of that content AND the publication or website allows you to re publish your content.
VERY IMPORTANT: Any content you submit should NOT have any patient or subject identification in any shape, way or form. For example, when you scan or photograph a video or screenshot, please make sure the patient identification. including name, medical record number, date, location or name of facility are NOT visible at all. This is a strict requirement in keeping with HIPPA privacy rules and there are no exceptions. Content identifying any information that remotely leads to recognition of the patient identity will NOT be published on this forum.
NO RENUMERATION: Since this is a voluntary and strictly non profit venture, we will not be reimbursing for any content published here. What we present here is for imparting knowledge and teaching students and residents and practicing physicians world-wide and we do not expect any monetary reward, other than thanks. If any money is made will be spent in maintenance of the domain name and server. At present, it is being paid from the personal funds of Amin H. Karim MD.