By Amin H. Karim MD Joseph Aaon MD (Interventional fellow) We present a case of acute myocardial infarction with total occlusion of the left anterior descending coronary artery. A 85 year old male presented with several hours of atypical chest pain. EKG at a free standing ER showed ST elevation in the antero-septal leads. Catheterization was done in the 90 minute door to balloon time and showed the following: There was a vessel alongside of the left anterior descending coronary that looked like a bridging collateral. Our question was: is this a chronic occlusion with a collateral or was it an acute occlusion causing the chest pain and EKG changes. Orthogonal views were obtained to make sure we do not end up wiring the bridging collateral, which may give the impression of wiring the true lumen. hence it may not hurt to obtain one or more orthogonal views to confirm the position of the wire. The micro catheter also helps if there is confusion. Injection of the contrast into the vessel can differentiate a bridging collateral from a branch of the vessel.
The lesion was crossed using a micro catheter and a whisper wire. 3.5 x 38 mm DES was placed. Final result was satisfactory.
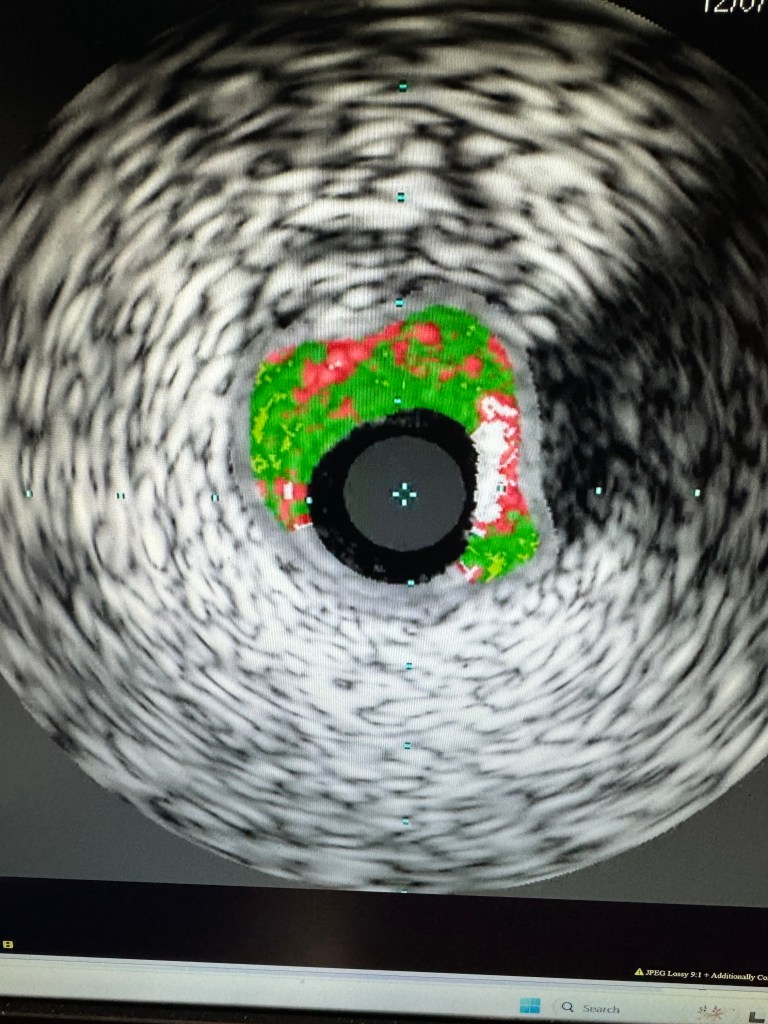
IVUS pre dilatation showed a fair amount of calcium.
Echocardiogram obtained the next day showed anterior wall and apical akinesis. There was a layered thrombus in the apex of the left ventricle. Patient was anticoagulated with warfarin, in addition to clopidogrel and aspirin. Plan was to discontinue aspirin in 2 weeks to reduce the risk of bleeding.
By Amin H. Karim MD In 2014 while on STEMI team call I admitted a patient a 56 year old medical researcher, to the Houston Methodist Hospital with severe chest pain and EKG changes of an anterior wall myocardial infarction. He had lost his pet cat 2 days before and was sad. Cardiac catheterization done as an emergency showed normal coronaries with an akinetic apex. He was treated as a case of stress induced cardiomyopathy, the stress in this case being death of his pet. He is lost to followup.
In 2018, I admitted a 54 year old lady status post cardiac arrest, again showing normal coronaries and severely depressed left ventricle. There was mild coronary artery disease, in no way accounting for the wall motion abnormalities on the left ventriculogram. She too had lost her pet cat a day or two ago resulting in severe anguish. She underwent placement of an Implantable Cardioverter-Defibrillator (ICD) and is doing well 5 years later. Her left ventricle has recovered completely.
These 2 cases were written up by our observer medial residents from Pakistan and China. It was published on Cureus and is posted below:
By Humayun Naqvi MD , Interventional Cardiologist and Salman A. Arain MD (Associate Professor McGovern Medical School at UT Health)
A 56 year old man presented to Dr. Naqvi with angina in 2021. Cath showed multivessel CAD and underwent CABG with LIMA to LAD and vein grafts to OM and Diagonal. The RCA was not bypassed.
He presented in June 2023 with worsening angina despite optimal medical therapy (OMT). Here are angiograms:
LIMA was patent and filled the distal LAD; OM graft was patient suppling a small territory. Diagonal graft was not visualized. RCA which has not been bypassed was occluded. Patient was started on optimal anti anginal therapy with isosorbide mononitrate, ranolazine, metoprolol, amlodipine, and aspirin. His angina resolved reducing the need for sublingual nitroglycerin. The question was what to do next: The choices were: Optimize GDMT and pray for the best Consider EECP (and GDMT) Viability study +/- judicious PCI Viability study +/- re-do CABG LVAD evaluation Look for experimental therapies, e.g. myocardial laser or stem cell therapy. Here is our thought process: The most common symptom in patient with CTOs and significant ischemia is dyspnea (and not chest pain). The reason for the ‘graft failure’ in this patient is a discussion in itself. (They did not fail as you will see). We typically like to determine viability, ischemic distribution, and burden before embarking upon complex PCI. Here the strong possibility of balanced ischemia and the angina despite a hefty anti anginal regimen, made us choose PCI first. The plan was to perform a PET after ‘unbalancing’ the ischemia…
There is significant ischemia in the RCA territory. We decided to work on his native coronaries and ended up with stents in the ramus and LCX. POBA in the LAD. I like to use a technique called JSBT or JSKBT – jailed semi-inflated (kissing) balloon technique. This is the absolute best way to preserve side branches. 👌🏼Here are the final images:
You can see that the diagonal graft fills retrogradely and was therefore open. Also there is a blush in the distal RCA territory signifying later remodeling or vessels and collaterals. Patient is followed by Dr. Naqvi and as of December 2023 seems to be doing well with significantly less effort angina and return to a decent lifestyle.
Essay edited from WhatsApp messages by AHK. December 9 2023.
QUESTIONS: Some questions raised by the readers: ” ood technical case. May I ask the question, if angina resolved with medical therapy with less use of NTG, what was the wisdom for extensive stenting at that point?” Second: ” Thanks for the share. From a percutaneous perspective, the SVG to OM was widely patent and most of the ischemia was inferior. So what was the rationale of doing LM into LCX PCI before RCA? Wasn’t RCA PCI alone indicated/enough?” I advised entering the questions in in the blog itself which has place for discussion so it could be answered there. ANSWERS: Dr. Naqvi: The angina did not completely resolve. He was needing to take 2-3 pills of nitroglycerin on top of all the medical therapy, extremely fatigued, and the episodes of angina 2-3 times a week was anxiety provoking for him leading to an ER visit as well. That’s why he was referred for PCI. I saw him yesterday in the clinic for follow up and he was almost in tears thanking us. He said he hasn’t felt like this in years and has so much more energy. He is back at work, active, and doing more physical work. Worked in his garage the whole day without a problem.
Dr. Salman Arain: Good questions. Here are the answers and a comment: Most patients with a CTO and significant ischemia (>15% or more) do not have angina. They have exertional dyspnea and fatigue which can be lifestyle limiting.
The stress test was after the LM PCI. Also, most guidelines and experts favor treating the donor arteries (and any non CTO lesions) before addressing the occlusion. There were left to right collaterals and we were under the impression that a graft to a major diagonal had gone down.
Now for the comment. CTO PCI is done for quality of life not survival. There is some data from Lance Gould using PET that the degree to which ischemia can be reversed has an impact on mortality. But we haven’t been able to connect this mortality benefit to CTO PCI.
But there is more to life than just longevity. Fixing a major CTO (like this one) can have a major impact on QOL. And reduce the number of medications needed. Of course, it doesn’t replace the need for essential GDMT.
I tell my colleagues that CTO PCI is a bit like doing knee surgery for someone with bad joint disease. Does it prolong life? Not at all. But you don’t have to rely on crutches any more, and you become more mobile. Of course, you still need to lose weight, go through rehab etc. Obviously, this is a biased perspective, but it is supported by my experience of treating CTOs of the past five years. Patients can and do feel a major difference. I almost always do some type of functional test so that the pre-treatment probability of benefit is high.
BTW, here the purpose of the PCI was also to finish the job that CABG had started – complete revascularization. Interestingly, many of my patients are post CABG.
Tons of great interventional content! Thought I’d add some EP:
Who doesn’t hate vasovagal syncope? Usually, younger patients with little comorbidities, lifestyle changes aren’t always effective, and pacemakers help the HR but the patients still feel poorly. Then young pts have to deal with PPM gen changes, lead issues etc.
Had been doing this in Chicago for a bit, now in Houston: Cardiac Neural Ablation (CNA)
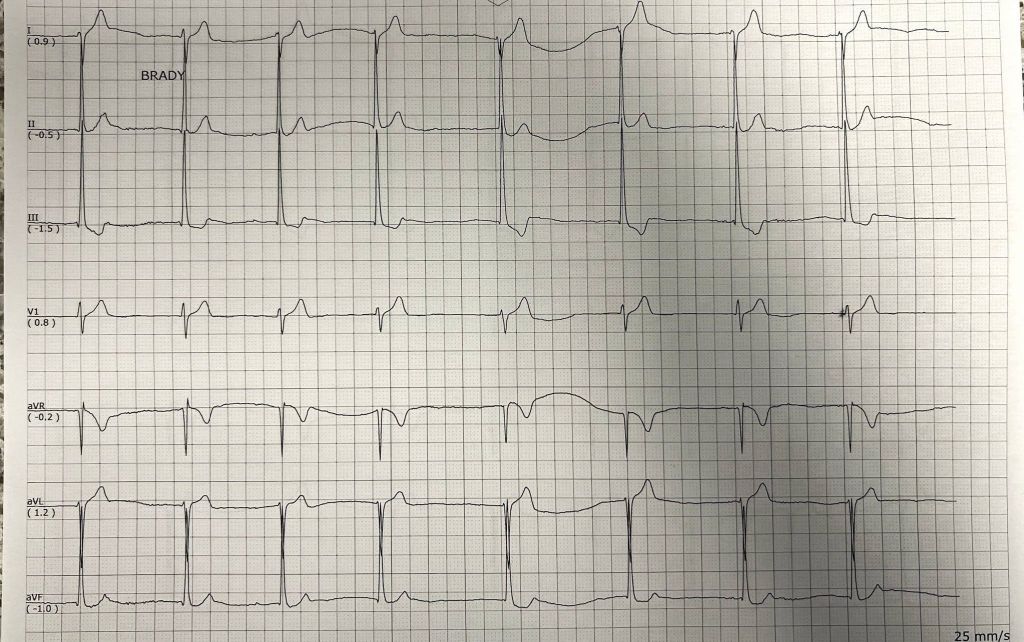
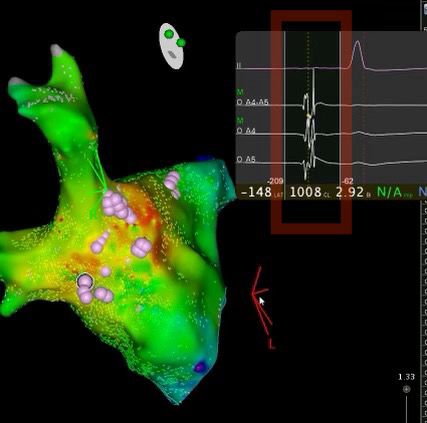
Male pt Mid 30s pt with multiple episodes of VVG syncope, no offending meds, documented drop into junctional with sx. Resting Brady. Referred for pacemaker. One of the screening tools, is giving 1mg atropine to see if there’s a ⬆ HR by at least 10 bpm. He qualified. Took him to EP study. Very detailed electroanatomic map of RA, LA, looking for high fractionated signals in usual anatomical spots posteriorly indicating presence of vagal plexus. Ablation in this area shows response of ⬆ HR during RF 🔥. End point: lack of atropine response. Then clinical observation for sx. Upto 4 patients in Houston now, no recurrence in syncope. None required pacemakers.
My group is part of the international research registry for such pts. Technique recently popularized by Turkish EP in Istanbul: Tolga Aksu
Pics: ECG with sx, Left Atrium with Pink dots = area of burn. The high frequency signals that signature vagal plexii are in the red box, that we hunt for…
once you have vasovagal syncope narrowed down by excluding everything else, removing offending drugs, these are good referrals for further work up
it’s always nice to have outpatient monitoring correlating sudden bradycardia with symptoms
a screening tool that I have, baseline, ECG, then IV 1 mg of atropine, With repeat, ECG, you want to see a change of at least 10 to 15 bpm increase in heart rate (these patients benefit most)
a positive test for a cardio inhibitory syncope is also helpful for the record and to get pre-authorization
there’s no age range, per se, but these patients tend to be younger, which is a reason for me to try and find a way to make them avoid hardware, specifically a pacemaker
my last patient interestingly had resting bradycardia and was on fludrocortizone and compression socks, and very interestingly, almost immediately he was able to come off both measures and took his first fishing trip in five years
A few times, with only a outpatient monitor, showing bradycardia and symptoms, then after mapping, the vagal plexus, with subsequent rapid bursting to stimulate the vagal response was the only way I could prove they could benefit — intra procedure testing… sometimes you just have to prove physiology intra op, just like utility of IVUS, FFR etc…
By Amin H. Karim MD Parth Desai MD (Interventional Fellow)
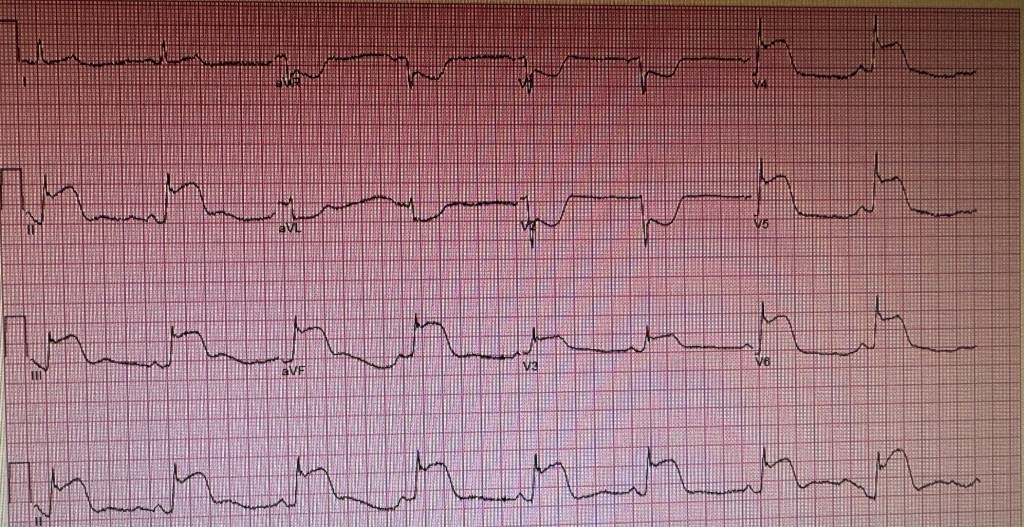
CASE REPORT: A 61 year old Caucasian female presented with sever chest pains for 3-4 hours. EKG was obtained.
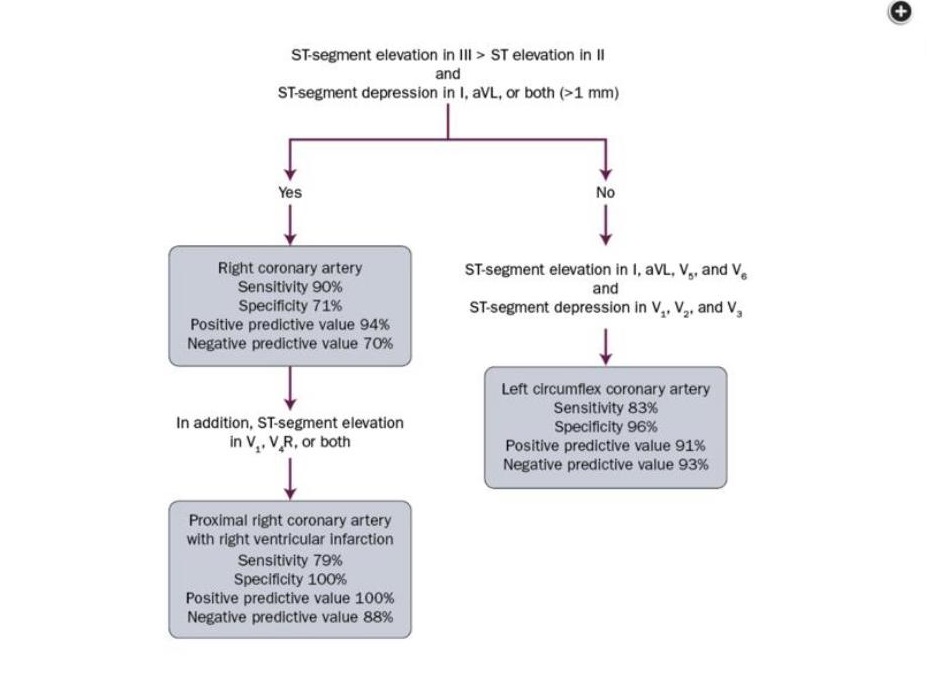
We put it through our panel to see if they could figure out the location of the culprit lesion in this STEMI patient. The answers ranged from a large dominant circumflex or RCA to a combined lesion in the LCX and LAD. Take a moment and see if you can tell the location of the lesion. Perhaps you can use the chart that was went by Dr. Syed Fazal:
Cath showed the following:
A subtotal occlusion of the left circumflex coronary artery before the obtuse marginal takeoff. It does not look that this distal circumflex supplies the anterior wall or the apex of the left ventricle.
Here is the view of the LAD (Left anterior descending) coronary artery showing there is no obvious lesion or any cut off to suggest that there may have been a clot in the artery which would have caused the anterior wall changes in the EKG.
We crossed the LCX lesion using a whisper wire, pre dilated it and placed a 3×18 mm Synergy DES with a satisfactory result.
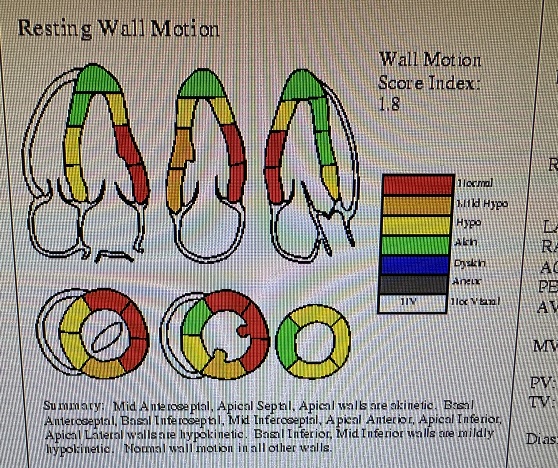
So the question remains, why the extensive changes on the EKG when the lesion is localized and one would have expected changes in the inferior or inferior and lateral leads. Could the patient have a hypercoagulable state? malignancy?. There is no evidence of spontaneous dissection. Concomitant spasm in the LAD with the thrombus in the LCX is a possibility (reported by us in 1990’s and the two published articles are on this website). her troponins peaked at 8500. Echocardiogram showed wall motion abnormalities as follows:
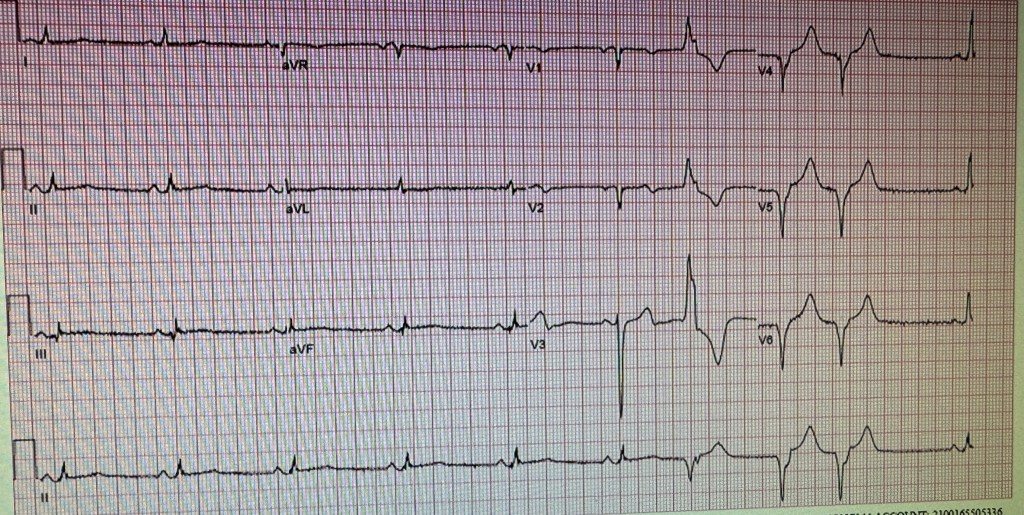
EKG done the next day. Patient did well clinically. The global ejection fraction was 45-49%. Incidentally patient also took Adderal of and on for attention deficit disorder. There are reports that these drugs can increase the incidence of cardiovascular events. INDEBTED TO COMMENTS ON THIS CASE BY: Prof. Salman Arain Dr. Syed Arman Raza Dr. Farhan Katchi Dr. Zubair Mohammad Syed Dr. Syed Fazal Dr. Usman Mustafa
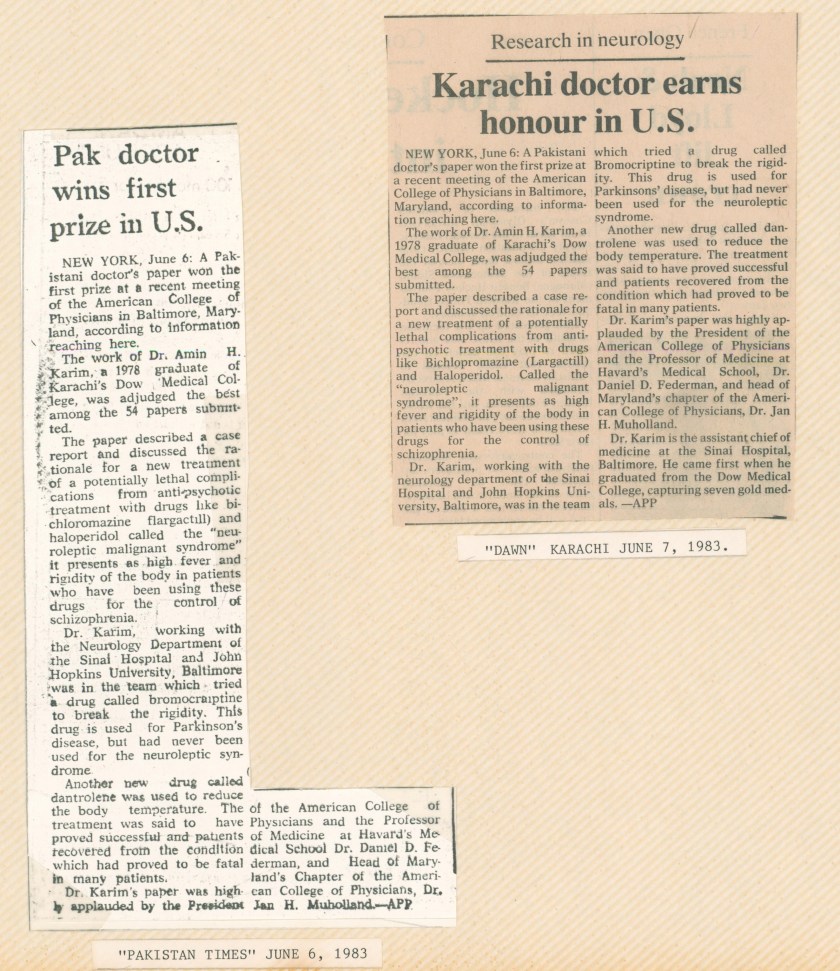
Neuroleptic Malignant Syndrome: Successful Treatment with Dantrolene and Bromocriptine. By Amin H. Karim MD
1982: Sinai Hospital of Baltimore, Maryland. As a second year Internal Medicine Resident I encountered a patient with high fevers (as described in the article) After discussions and neurological consultations we came up with a plan of treatment that had never been tried before and it proved to be successful and the patient fully recovered. The article was published in the Annals of Neurology Vol 14 No. 1 July 1983; It has been cited many times in the literature over the years. I presented it at the Young Investigator Conference of the American College of Medicine in 1983 and it was adjudged as the best presentation.
Dr. Barney J. Stern MD, Neurologist and Co-author of the article.
1983: With Dr. Allan Krumholz, Chief of Neurology at the Sinai Hospital of Baltimore.
Arteriographic Demonstration of Coronary Spasm During Thrombolysis
By Amin H. Karim MD
In 1986 I was a Cardiology fellow at Baylor College of Medicine. Our cath attending at the V.A. Houston Hospital was a Frenchman Dr. Jacques Heibig, a young cardiologist with his own approach to Cardiology training. We would do 6-7 cases in a single cath lab room. Time was of the essence. He would make us do a quick job and expected us to finish the case in 10 minutes. There was no angioplasty at the time at the V.A. We would do thrombolysis for acute MI using TPA (or blinded to TPA versus Streptokinase when the patient was assigned to TIMI 1 protocol). The TIMI 1 patients would be taken to cath lab within 90 minutes as part of he TIMI protocol to assess if the culprit artery was open and reperfusion established. In the process, we discovered that some patients would have spasm in the partially re-perfused artery prompting me to write up a case report. Two years later we would publish another more formal case report with Dr. Raizner and Dr. Chahine. Dr. Heibig later moved away from Houston.
Dynamic Coronary Thrombosis: A possible cause of Prinzmetal’s Variant Angina.
By Amin H. Karim MD Dr. Albert E. Raizner was the Director of Cardiac Cath Lab at the Houston Methodist Hospital while it was still affiliated with Baylor College of Medicine and even after it dissociated from Baylor. He was my teacher when I did my Cardiology General and Interventional Fellowship at Baylor College of Medicine, Houston, Texas. He and I were very interested in coronary spasm in the days when thrombolysis was the primary treatment of acute coronary syndromes; it would be followed by “rescue” angioplasty if the ST segments remained elevated or there was post infarction angina or residual ischemia. We would come across cases where there was spasm in the coronary artery even without the diagnostic catheter tickling the intima. This lead us to surmise that maybe the presence of thrombus in the artery itself caused the spasm. The paper, we co-authored by another researcher of coronary spasm Dr. Robert A. Chahine, University of Miami School of Medicine, Florida, was published in the Journal of Interventional Cardiology, Vol 3, No. 1, 1990. Dr. Raizner is now semi retired.
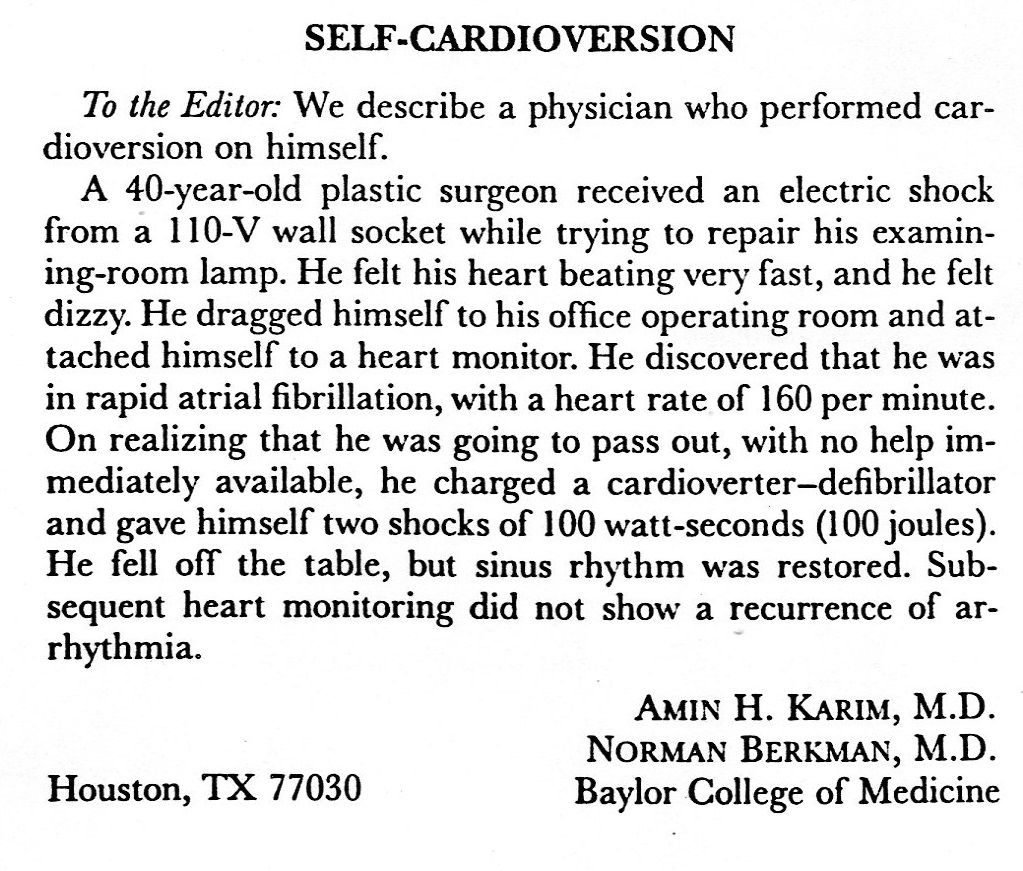
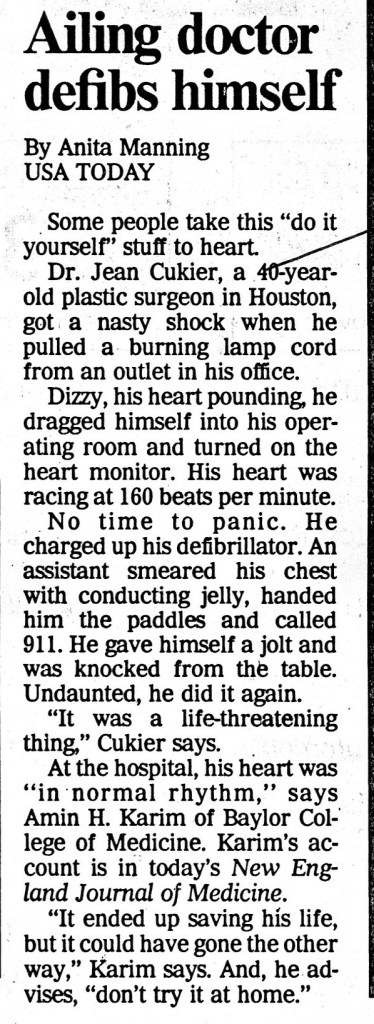
1995: An interesting encounter took place with someone I knew. The case was reported in the New England Journal of Medicine March 2, 1995. The case generated a lot of publicity with coverage on TV and newspapers. We even got a call from ABC Network for an interview on air, but the doctor declined. He recovered with no sequelae and went back to practice, retiring recently.