Heart health apps typically target the most common types of CVD, including arrhythmia, heart failure, and coronary heart disease. However, there is a general lack of scientific evidence for the usability and clinical potential of heart apps. They can be useful for the patient to monitor at home and give them an incentive to maintain their heart health. Some popular heart apps include:
CardioVisual: This app is educational in nature. It has shareable videos with a wide variety of content aimed at both clinicians and patients. It allows connectivity for coordination of care.
Heart Failure Storylines: This app from the Heart Failure Society of America is a tool patients can use to track daily vitals, medications, symptoms, and more, and share it with their care team.
Instant Heart Rate: This app uses the camera phone to measure heart rate through the fingertips. It graphs results and can provide printable reports patients can share with you. Its accuracy has led to partnerships with entities such as University of California San Francisco.
KardiaMobile: This app pairs a smartphone with the FDA-cleared KardiaMobile device. It takes an instant EKG and can detect common arrhythmias, including atrial fibrillation. Data can be tracked over time and shared with the patient’s care team.
Qardio: This app works exclusively with Qardio devices to track heart health information, such as heart rate and blood pressure. It is shareable and can pair with smartwatches.
Smart Blood Pressure: This app replaces a written journal for tracking blood pressure, pulse, and weight. It can sync with Apple Health or Google Fit and provide shareable reports.
In 1987, I was approached by an attorney firm to take care of patient who was under trial. I did and next thing you know is a subpoena from the Court to present in the courtroom to give a deposition in front of the Judge. The proceedings are all public records. Later, the attorney (not mentioned in the article) herself became my patient.
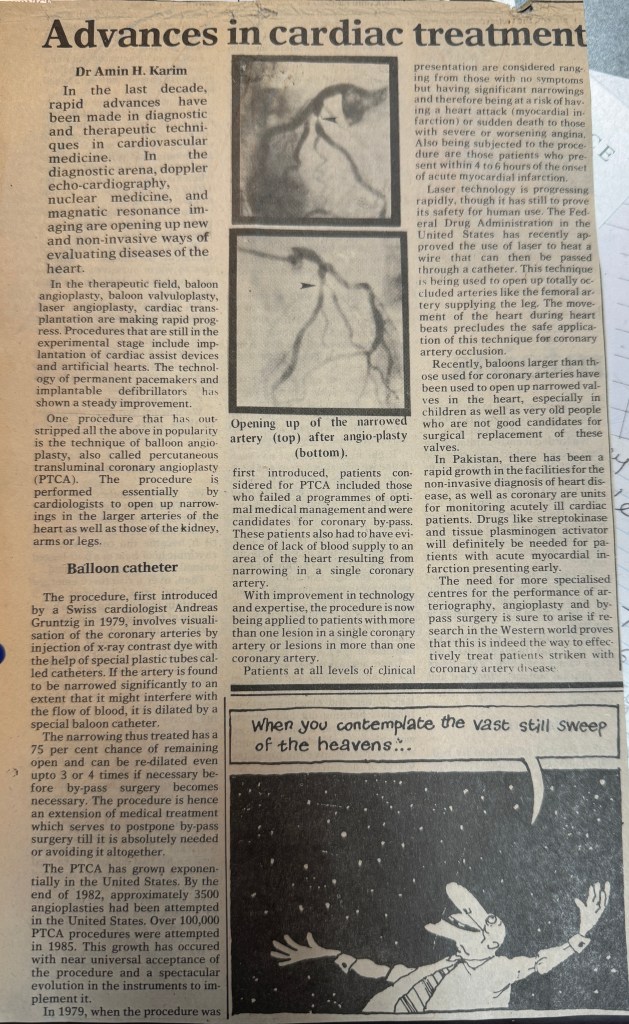
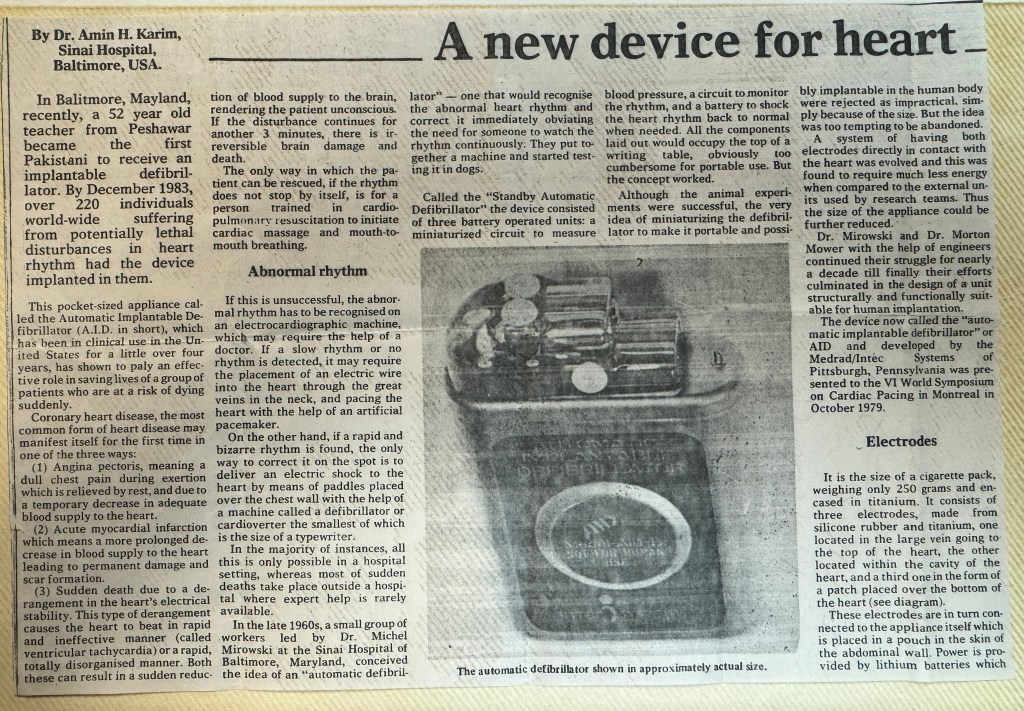
By Amin H. Karim MD This article was published in 1986 in “Hospital Practice”. May still be applicable since trimethoprim-sulfamethoxazole is still in use when indicated for infections susceptible to sulfas.
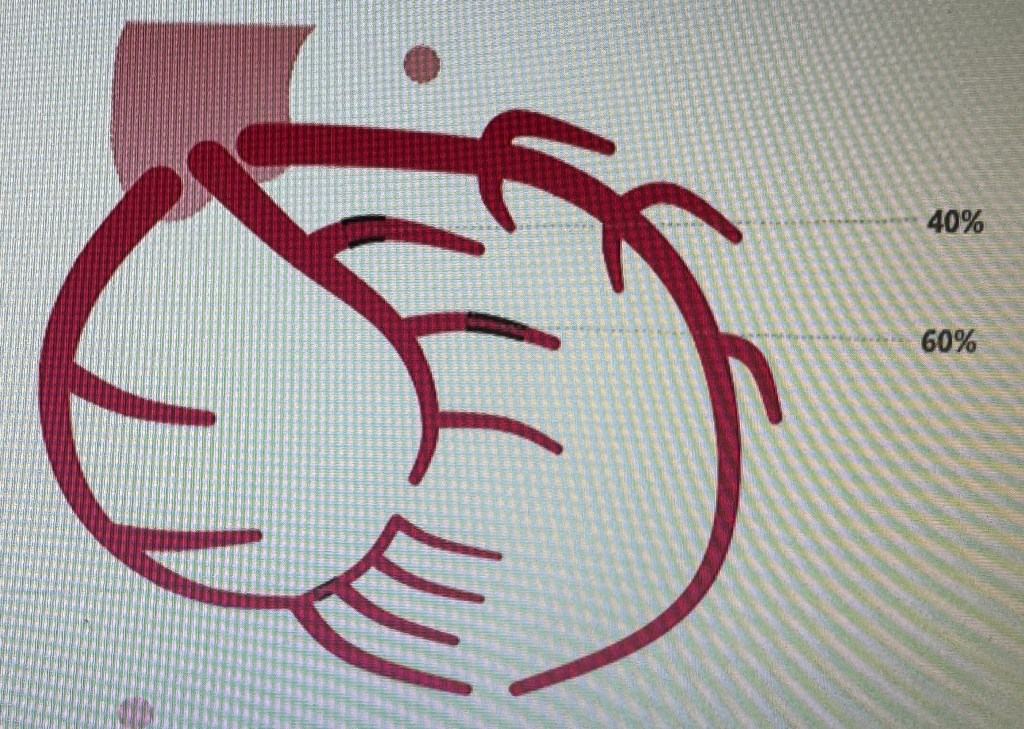
Andreas Roland Gruntzig used to say “ other cardiologists wear a surgical cap for sterility, I wear mine for style” ( Spencer King) In the late 1960s, Gruentzig learned of the angioplasty procedure developed by Charles Dotter, an American, at a lecture in Frankfurt, Germany Gruntzig did the first balloon angioplasty in 1977 in Zurich on a LAD focal lesion using a balloon devised in his kitchen. Gruentzig presented the results of his first four angioplasty cases at the 1977 Amrican Heart Association (AHA) meeting, which led to widespread acknowledgement of his pioneering work.
10 years later Cath at Emory in the patient showed a patent LAD. Gruntzig passed away October 27 1985 in a plane crash in Georgia with his wife. ( October 27 1958 Ayub Khan took over Pakistan!). “ Gruntzig stated: “No matter what happens to the technique, I have made one contribution, and that is allowing physicians to work within the coronary arteries of the awake, alert patient.”
Gruentzig’s success remains a major breakthrough and great contribution to the field of medicine in demonstrating that doctors could work inside of the arteries safely, without the need for open surgery. By utilizing the arterial circulation as a “therapeutic highway”, many types of devices and drugs can now be delivered directly to the heart, kidneys, carotid arteries, brain, legs and aorta without the need for major surgery and general anesthesia.
A 72 year old dentist presented with several months of increasing shortness of breath. Echocrdiogram is as follows:
Severe left ventricular hypertrophy
Echocardiogram showed global ejection fraction of 50%; Grade III diastolic dysfunction with restrictive LV filling pressures; PA systolic pressure of 65-70 mm Hg. a specled appearance of the myocardium consistent with cardiac amyloidosis.
Coronary angiogram did not reveal any occlusive coronary disease.
Right ventricular endomyocardial biopsy showed a variable deposiiton of acellular material within the interstitium and replacing some myocardial fibres. Congo red stain and fluorescence microscopy with the Texas Red filter demonstrated strong positivity further supportive of amyloid deposition. The paraffin block was sent to Mayo Clinic for amyloid subtyping. it showed findings most consistent with age related amydoidosis since it did not detect amino acid sequence abnormality in the transthyretin protein.
November 2023: Four years after the above diagnosis patient is stable on treatment. He has a implantable automatic defibrillator and the current global ejection fraction is in the 45-50% range.
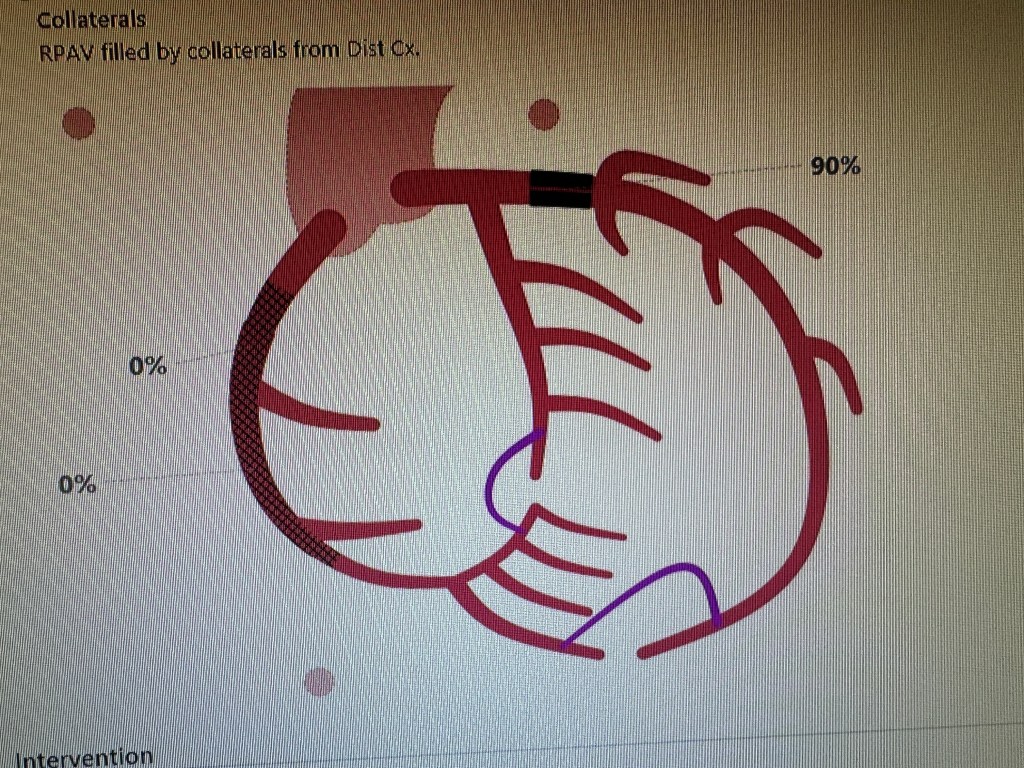
by Amin H. Karim MD Here is a case of the Left Circumflex coronary artery arising from the right sinus of Valsalva. (Type I anomaly). This happens in 0.3-0.6 percent of cases. Patient was a 42 year old lady presenting with atypical chest pain. The anomaly is usually benign but can be associated with non atherosclerotic coronary artery disease and myocardial infarction.
Left anterior descending coronary artery
Right coronary artery arising from its own ostium
The left circumflex arising from the right sinus of Valsalva separately ( Type I)
There is moderate occlusive disease in the branches of the left circumflex and the posterior descending coronary artery. It was decided to treat medically. The anomaly brought to memory the pre-stent days of plain balloon angioplasty. We had a similar case in the 1980s presenting with unstable angina. Cath showed the anomalous origin and an ulcerated plaque in the body of the circumflex. We proceeded to do balloon angioplasty. Unfortunately, the artery dissected. We knew as trainee fellows that this was bad news. There were many measures which interventional cardiologists took to “tack up” the intimal dissection and restore the flow to the artery. Most common first attempt was to advance the same balloon back and try longer inflations as much as the patient could tolerate watching the ST Segments and the blood pressure and listening to the patient. If that did not work we tried larger balloon with low pressure inflation. In some cases it would make the dissection worse but worked sometimes. Some attendings would would try to find where the dissection started proximally and start dilating there. In any case, the procedure would go on for long. Late Dr. John Lewis would get suggest that this was all “inflammation of the artery” and would give ibuprofen to the patient. When this would not work and the artery would look more messed up he would say that “there is more trouble in the artery than in the middle of downtown Beirut” keeping in mind there was war going on in the Middle East at the time. In the meantime, the irate cardiologist who was to follow in the same room would be watching from the glass partition. And the good cardiovascular surgeons who graciously gave us “surgical backup” (mandatory in those days) would be waiting in the wings to see when we got tired to let them take the patient to the OR and operate….. 🙂 Those were the days….. (Amin H. Karim November 30 2013)
This is continuing of the Journey in Private Practice starting from July 1987 and onwards. Marketing efforts for a specialist (non primary care) solo practitioner whose only source of patients is either patient referral, word of mouth, social media, or some other colleagues in primary care, is a ongoing process that has to go on as long as the practice has to continue. This is especially try in a competitive area. Here are some other ways which AngioCardiac Care of Texas employed to remain in focus.
WRITING IN LAY PRESS: This is not difficult to do. Any public health topic can be addressed to help other people understand diseases and procedures available and prevention measures to be taken. It’s a noble thing to do, in any case regardless.
GIVING TALKS TO HOSPITAL MEDICAL STAFF: One gentle way of marketing effectively involved giving a Cardiology talk to hospital medical staff or primary care physicians, whenever an opportunity came forward. Topics would include Risk Factors, Screening for Heart Disease, New technology in Cardiology, topics that would interest them.
This section will recount in the journey some encounters with entities that representing venture (vulture) capitalists that come to town having done their homework which tells them that there are lot of dollars in the medical world. They also know most doctors are busy in their practices and have little time to look into other sources of income. So if they can be enticed into investing a little capital, sign up to work in the facility and get dividends they can have era income to supplement their practice income. Pretty simple concept and the share of limited partnership would conform to the Federal kick back laws. I recall some of these (all are in public domain). Some were very successful for all parties concerned and some not so successful, some never got off the ground an some utter failures were the physicians lost everything.
HIGHLY SUCCESSFUL! The one venture that has always impressed me and still does is the TEXAS ORTHOPEDIC HOSPITAL in Houston. in the early 90’s a large orthopedic group called the Fondren Orthopedic Group partnered with Hospital Corporation of America (HCA) to build a hospital dedicated to Orthopedic Surgery only with related entities like Radiology and Physical Therapy. There were about 20 partners in the group. I am not privy to what the financial arrangement was but word on the street was that the HCA would manage and operate the hospital in return for 20% of income and the rest would go to the Physician Partnership. The surgeons would use the hospital for most of their work. The model proved to be a great success. The hospital added a third floor and parking lot and continues to thrive with 50 plus orthopedic surgeon in one big group.
A second venture that proved very successful was the NORTH CYPRESS HOSPITAL on Highway 290 in Cypress. An entrepreneur made a mid size hospital with processional building and made physician own limited partnership interest in the hospital. The secret to their success was out of network billing which brought them huge profits and dividends to primary care and specialists who were partners and who worked at the hospital. For a while it worked till the savvy insurance carrier realized that patient with out of network benefits were preferentially being treated at the hospital. I think were lawsuits and not sure how they all ended. In any case the hospital was eventually sold to HCA System which now owns and operates the hospital.
A 85 year old dialysis patient who presented with non stemi last week; we stented his occluded RCA with good result and brought him back today for his LAD lesion; looked straightforward but the access to LM proved to be a challenge being on the roof of the sinus in a dilated aging aorta. The lesion itself looked juicy and inviting! 🙂 Iliac was tortuous so we ended up kinking a few catheters till we decided to beat it and go with the longest 7F sheath in the arsenal and a FR 3.5 came to our rescue. The rest was a piece of cake with predilatation and a Resolute Onyx Drug eluting stent 3.0 x 18 stent post dilated with 3.5 mm NC. According to Dr. Waqas Qureshi, MB guide would be another option in cases of wide aortic roots.
If one jumps into a solo practice, one of the first items on the agenda is how to market the practice. Back in 1980’s here is what I did. Things are bit different now but the samem principles apply:
Making friends with Primary Care Physicians: I made a list of as many primary care physicians in the area as I could find; target was independent physician offices and excluding those connected with the Medical Schools, VA System, County Hospitals etc since they were obligated to refer within the system. When time allowed I would visit each one of them and provided they were not busy with patients meet with them and leave business cards. Remember the 3 words that someone taught me a long time ago: be AVAILABLE, ACCESSIBLE AND AFABLE! Not all PCPs are easy to convince and break away from the usual referral patterns or ” buddy networks” but even a few breaks are welcome and once you start working with them and impress them with your communication and good care, you may get a long term referral source. More convincing is if the patient goes back and says good things about you.
Arranging an talk at a restaurant on a cardiology topic that would interest other physicians. This would take some investment or if one is lucky a drug rep might offer to underwrite the expenses. This is as long as they understand that your talk will be unbiased.
Buying an infomercial on local TV or radio. Luckily I was approached by a Spanish TV station to be interviewed by an anchor and answer questions on cardiac topics. Same with local radio stations. This gets your name out in the community.
Organizing special events: (1990s) Here we learned something from Prof. Denton Cooley. Although, Dr. Cooley was full resident of St. Luke’s Episcopal Hospital, and on faculty at the University of Texas, Houston and founder and Chair of the Texas Heart Institute, but in fact he was a private practitioner just like the rest of us independent cardiologists. He has about 6 partners in his practice and he had an exclusive arrangement with St. Luke’s such that no other CV surgeon could have privilege to do surgeries at the hospital unless they joined his practice. It was rumored that even Dr. Michael Reardon, who was his fellow, got independent surgery privileges at St. Luke’s. As a result, Dr. Reardon ended up going to next door Methodist Hospital ( a big gain for Methodist as Dr. Reardon established a very good practice and continues to be a busy CV surgeon at Methodist. In any case, Dr. Cooley excelled in marketing his practice. A cardiologist Dr. Virendra Mathur, was his referral and with him Dr. Cooley would visit Bombay, India and meet cardiologists there, ensuring a steady referral from India. As expected, these referrals would be well to do people or VIPs paying cash to St. Luke’s. (which had a good cash pay program for overseas patients). Personalities like Bollywood singer and actor Kishore Kumar and Pakistani nightingale singer late NoorJejan came to St. Luke’s for their CV surgery. So di many industrialists from Pakistan, some of who later became my patients once they found that there was a Pakistani descent cardiologist just next door to St. Luke’s. Locally, Dr. Cooley would organize a get together of his referral cardiologists every holiday season at his beautiful ranch in Rosenberg, Texas called the Cool Acres Ranch. It had streams running through it and 5 big houses. He would arrange a barbeque and fire works for children. We would have a good picnic at his ranch. It was friendship, camaraderie, marketing and goodwill all rolled into one and showed his talents, outside the operating room. He was a pleasant and friendly person who treated his colleagues with respect. His surgical skills do not need any praise as he was outstanding. In later years, he would not keep up with the advances in CV surgery like mini-cab with smaller incisions and off pump CABG, calling them ” mere gimmicks” ( as he once told me). But his legend, like that of Dr. DeBakey lives on at the Texas Heart Institute Building.
TAKING PART IN HEALTH FAIRS: One way to spread the word about your practice was to take part in Health Fairs, some organized by the hospital system, some by the local community associations (eg Association of Pakistani-Descent Physicians of North America APPNA South Texas Chapter) or the Islamic Society of North America (ISNA) or the Islamic Council of North America (ICNA) or the Pakistan Association of Greater Houston (PAGH). Photo below is the Health Fair in 1995 at the Women’s Hospital of Texas on Fannin Street.