
A Panel Discussion Between Practicing and Experienced Cardiologists
on How to Tackle Risk Assessment in Asymptomatic People .
The case presentation and the comments that follow were interchanged on our WhatsApp groups APCNATeam in November 2024. This discussion presents an example of how experienced practicing cardiologist, faced with real life patients, navigate the findings on trials and papers and come to conclusion of what to tell the patient and how to proceed with the next preventive or therapeutic step. Please excuse any errors or omissions and will be happy to correct since the readers are themselves the Editorial Board. (Amin H. Karim MD)
Dr. Bashir Hanif
Need opinion on a 45 year old with positive family history of premature CAD. Asymptomatic. Very active, brisk walk n jog 45 minutes 6 days a week without symptoms.
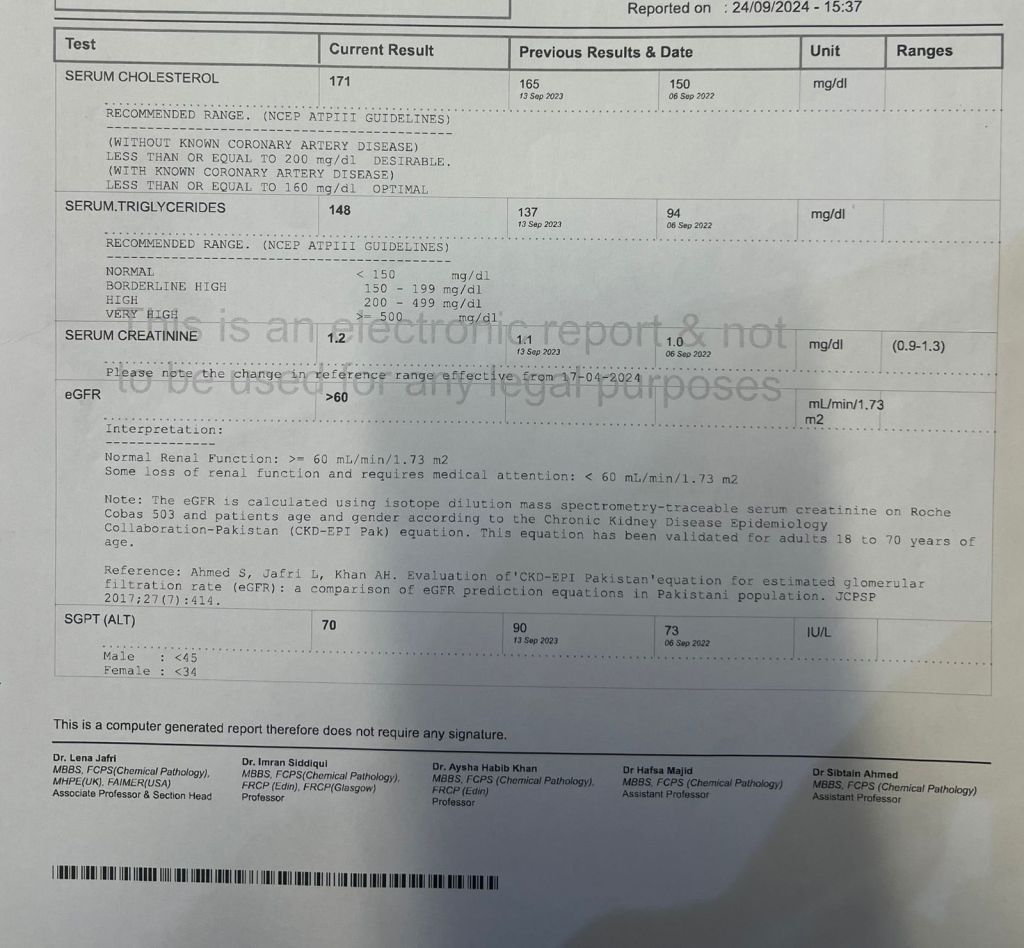
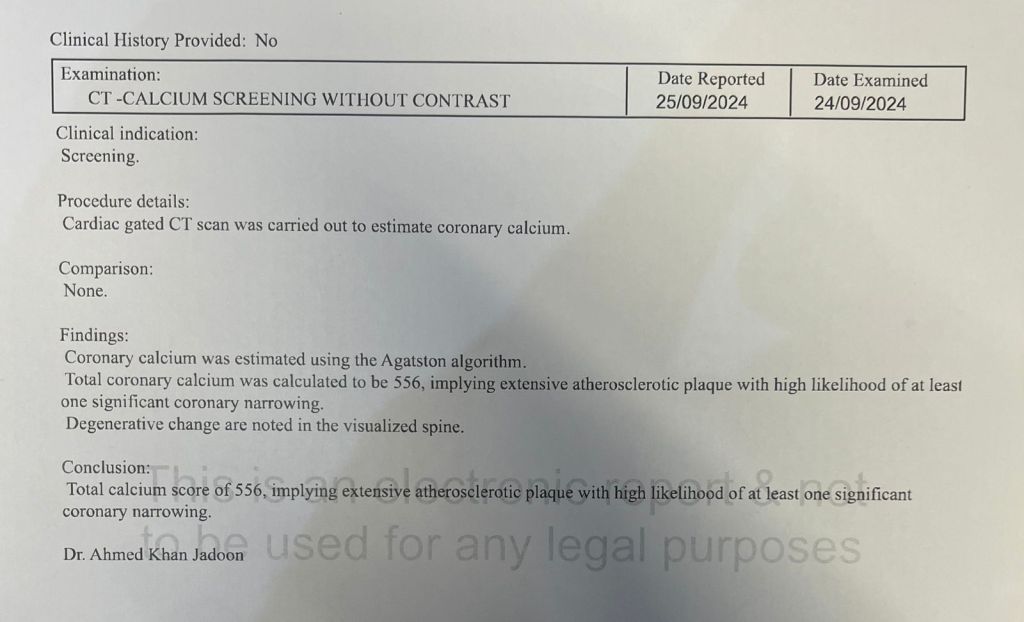
CAC n Lipids are given below. What would you do next? Cath? Stress test? Or just Aspirin n high dose statins?
Abdul Hakeem
Where is the bulk of the calcium? If it’s a prognostically imp territory then I would get exercise MPS for further risk stratification. Agree with HD statin bring LDL<50 perhaps EPA
Salman Arain
I had the same question @Dr.Basheer Hanif – what is the distribution of calcium? 550 distributed over three vessels is less concerning than 350+ in the LM and proximal LAD. In the latter case, I may offer a stress test. Also, if the patient has a family history of premature CAD, then it may be reasonable to do a stress test.
Maryam Moten
Hussain Khwaja
I would do ASA and high dose statin to bring LDL between 25-50
Question is what we are going to do if stress test comes abnormal ?
Basheer Hanif
That was my problem too as this was the only report apparently they gave which doesn’t give distribution of calcium. He is completely asymptomatic despite heavy exertion.
Abdul Hakeem
So how does calcium scoring help in a very active asymptomatic person? Just creates a very pesky conundrum
Khurram Nasir
Preventive Management my friend, think beyond stenosis and intervention
Muhammad Saad
it can help to emphasize use of statins in asymptomatic patients
Khurram Nasir
Ldl below 55
Check Lpa if high family screening
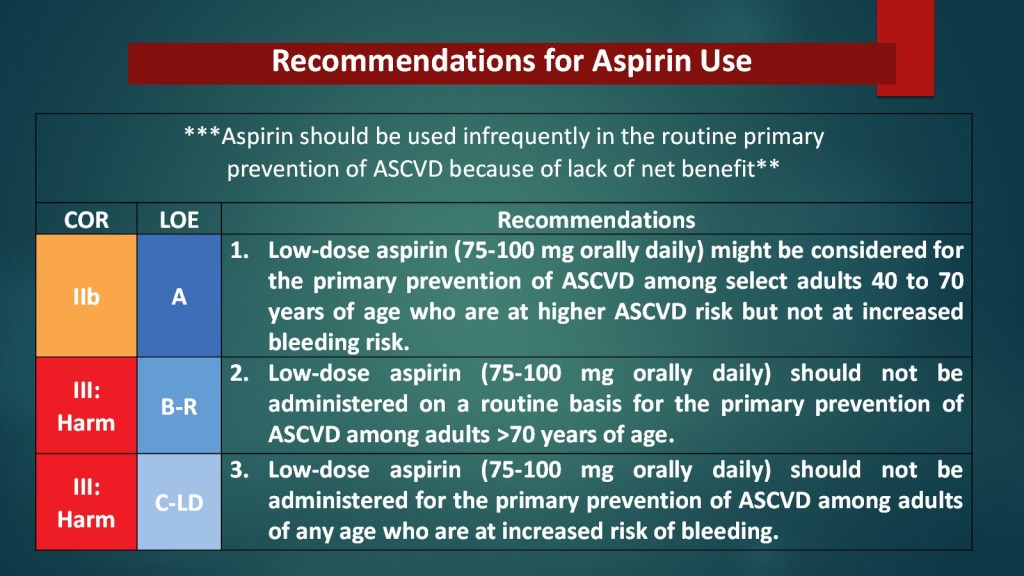
ASA
SBP below 130
GLP1RA if diab pre diab
Further emphasize on diet and lifestyle
Abdul Hakeem
I have heard that and I’m sure there is some piece of evidence that it modifies human behavior but the consternation it causes seems to be its overwhelming impact!
Khurram Nasir
Few thoughts :
Make sure they’re not capturing any MAC
paradoxically the more number of vessels involved the more risk (prognostically) vs the more rationale thinking that if higher in one vessel possibly higher risk of stenosis or future risk
the relationship of high cac is not correlated with the stenosis in the same vessel, actually u may find often in the other with less score
the issue is more distributive cac more turbulence in flow and more risk beyond plaque burden and rupture risk
despite higher risk, majority don’t have event so no good way to assess who specifically is more at risk
stress test not a bad idea in these uncertain cases
hopefully pak Sehat with cac and CCTA in young Pakistanis will tell us what it means so kudos to bashir on leading the way
There is now huge body of evidence, actually, there is a meta-analysis from our group and JCC imaging that higher cac modifies, patient lifestyle, behavior, and attendance, and as well as physician behavior on prescription patterns
Also, as thought, from rationale thinking that it may increase anxiety and concerns, apart from few anecdotal cases, actually the evidence suggest otherwise
I see these patients all the time, it is how you message to them, that is great that you found out this,rather than waiting for an event to happen, and we have simpler an easier way to significantly modify the risk
Abdul Hakeem
Calcium score (in hugely asymptomatic)= demaagh me keera. The pt will find himself a Cardiol who will be more than happy to cath and stent him ( to prevent events
Khurram Nasir
I believe you; Well, just because there are bad practices, and some of these arguments have been made by long-term skeptics like David Brown even in the US, doesn’t mean that we stop doing the right thing
it means we start educating not only the patients, but also Cardiology community on what the best practices are
This is like saying we should stop screening for hypertension, because most of cardiologist will start on clonidine and may cause more harm
The same argument it’s gonna be made for anything
For deemagh me keera means more patient discussion and education and that means spending more time at the patient, unfortunately, that doesn’t exist much in most place even beyond Pakistan, and maybe that’s what we need to do, so we have more patient centric approach and care..
And btw asymptomatic doesn’t mean the person is not high risk for MI not only long term but also short term
Can’t think of any good rationale why the pt and pts physician wouldn’t want to know about so actually one can mitigate this totally preventable catastrophic complications and downstream issues like revascularization
Abdul Hakeem
I can’t agree more. I’m just saying unless we have solid evidence that “screening ca scores” in healthy asymptomatic individuals alters long term outcomes incrementally to usual practice we should be selectively doing calcium scores particularly in prevention rebellious pts
Khurram Nasir
First of all, this is old school, and things have changed: Let me help, explain, also, we need to put yourself in the patient’s shoes and ask ourselves whether we are better off in making a guess or knowing the actual risk and personalizing management accordinglyly
Cac test is no longer a screening test but more of a decision aid to guide risk and management, screening means that you do it for a person who is not candidate for a therapy, you find disease, intervene, and see if it improves. Here cac is also used for a lot of individuals who are already candidates for therapy, is to guide whether they need it or not and what intensity, so completely different philosophy.
well proven to outperform any guesstimation approaches that you and Ion and others use in the clinic, and by the way, none of them have been tested in any randomized trial that using them improves outcome.. also by the way that I said I would be in a study that seeing a cardiologist improves outcome so maybe we can take everything with a grain of salt
as far as a pure screening approach and outcomes this concert there is a large study in Denmark, which is ongoing, and in the interim analysis has shhkwn 11% reduction in MI and stroke in the entire population, and three specified analysis, almost 11% all cosmetology reduction, and younger individuals
Abdul Hakeem
Thanks for the insightful comments khurram bhai. Always very scholarly and encyclopedic!
Syed Iqbal Rahmatullah
Repeat CAC to know the distribution or get the scan film to review.
High dose statin (goal LDL 30 to 40)
Aspirin
Lp a
Stress echo regardless of distribution
Life style adjustment. (Particularly dietary, HbA1c, BMI)
I had a similar patient yesterday, asymptomatic, played squash 5 days a week, and had very low LDL,
CAC 350, pakistani recently retired anesthesiologist, age 62, visiting his son here. No other risk factors.
SE showed anterior and inf wall hk, Rest echo 65%ef, post exercise 45%.
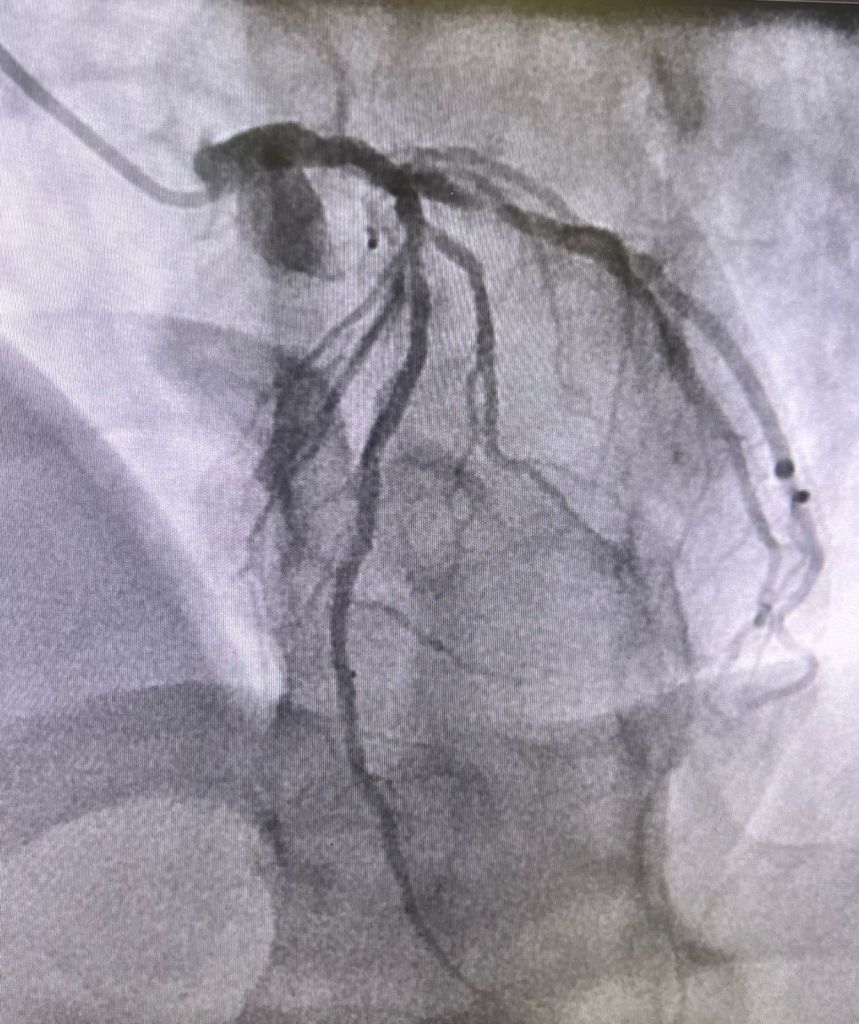
LHC showed discrete lesions but diffuse 3 vessel disease, extensive but good targets. Scheduled for cabg next week.
Farhan Katchi
I’ll just add that i use cac, as informed largely by Khurram’s body of work, and it has strengthened patient trust, buy in, compliance, and in my 7 years IMO better outcomes. My patients are more motivated to lose weight, eat better, exercise, and engage in escalating up medical preventative therapy when they know and understand the cac score concept (I show them the images in clinic on the screen so it’s concrete and not abstract). I have started to use LP(a) and ApoB in the same way that I use cac scores for risk adjudication, especially in women and the young where a cac of 0 may not tell the full longer term preventative story.
Bashir Hanif:



Syed Fazal:
Great discussion!
Now at the end of discussion, looks to like need one stent in type A lesion in mid cir, and all the above recommendations, for secondary treatment! Now he will need more anti platelets med for stent!
Bashir Hanif:
So who will put a stent and who would treat it medically. He is completely asymptomatic. It’s not a prognostic lesion!
Syed Arman Raza
Academic answer (in my view): no stent. Medical mgmt. Real world: stent + medical mgmt
Sabha Bhatti
Has he had functional testing ?If there’s ischemia in that territory you could consider stenting
Bashir Hanif:
You know functional study is going to be low risk and we are not going to change his prognosis/ risk of MI or mortality by putting a stent!!
Sabha Bhatti:
Yes but … Potentially that’s the bridge between academic and real world answer .. you have another justification for not stenting if there’s no ischemia
Bashir Hanif:
There will be ischemia. I can tell you what functional test is going to show. He jogs for 45 mins without symptoms. So it’s probably going to be medium size mild intensity ischemia at high work load. Will you send him to Hakim for stenting with this report?
Sabha Bhatti:
No one can do 45 min on a Bruce . Infact 16 min and few sec is the max I’ve seen . It helps to see symptoms , ECG and ofcourse vitals with exercise. No stent for now . Avoid oculostenotic reflex
Bashir Hanif:
I didn’t say 45 mins Bruce. I said jogs n brisk walk for 45 mins.
I advised him medical treatment. No stent
Ata Qureshi
This is a non prognostic, low risk lesion and I would manage it medically.
Syed Iqbal Rahmatullah
Bashir, was FFR done on left circ lesion? What was the rationale for doing cath, to begin with?
Bashir Hanif:
My point is it’s a non prognostic lesion pt is asymptomatic. Even if it had shown some ischemia or FFR was positive, in asymptomatic pt , would stenting change the risk of future MI or mortality??
I believe in CCS but if pt is symptomatic on GDMT or it’s a LM or may be Ostial LAD I would go for invasive approach and revasc. options. I don’t know about you and Hakeem but I had to relearn medical management of CCS when I moved back as lot of patients refuse to go for Revasc ( even LM n 3 VD ) and they are doing fine on medical management for years now. So as you said we need to resist oculostenotic reflex as much as possible!!( Disclaimer: I am an Interventionalist)
My 20 years of experience in Pakistan tells me Medical management can do wonders if done appropriately with belief!!
Abdul Hakeem
One our fellow intv cardiologist has classified this very well. Reasons for PCI in SIHD
if I can’t do it then GDMT
If I don’t do it someone else will
medical therapy until I return from vacation
Syed Fazal
I think most of us IC do lot more stents without evidence of mortality benefit.
Definitely there are regional differences for many other obvious reasons in different countries.
And as I said there is no consensus in this type A lesion.
Definitely in board exam don’t even think about stenting at this lesion!
Farhan Katchi
In cases of high cac, if I suspect LM or 3VD, I will Cath or CCTA to define anatomy for cabg referral. EXCEL and NOBLE and guidelines support revasc of this disease with cabg on account of its survival benefit even in asymptomatic patients. Now the ven diagram of asymptomatic and severe LM and significant 3VD is probably tiny especially if you consider 3V ischemic rather than anatomic disease and verify “asymptomatic” status on a treadmill
Haris Riaz:
I haven’t had a chance to follow this interesting discussion but ISCHEMIA trial frequently gets cited [sometimes even by people who haven’t actually read the full text or gone through the supplementary materials from nejm]. It might be interesting to note that:
One fifth patients in the conservative arm underwent revascularization
There are many other important limitations that need to be kept in mind before applicability. The trial [like COURAGE] reaffirms that medical management is effective in stable patients with stable symptoms compliant with GDMT.
Approximately one third of patients in ISCHEMIA had no angina in the last month before enrolment.
15% patients in ISCHEMIA had no objective evidence of ischemia on core lab assessment
One fifth patients in the invasive arm didn’t undergo revascularization
