By Dr. Arnav Kumar MD, MSCR Interventional Cardiologist HCA Medical Center Hospital Houston, Texas
87 year old extremely pleasant, active woman was sent to us for complex LM PCI . She has distal left main 70% disease, ostial LAD 70% disease, calcific 90% disease of the proximal high Obtuse marginal artery and 99% Proximal LCX disease.
The left main itself is very long and anomalous. We anticipated challenge in delivering equipments across the retrofelxed LCX. Additionally, she has distal RCA disease . She was felt to be too high risk for CABG due to advanced age We were able to cross the ostial LAD – lesion using a sion blue wire. We were able to cross the high OM lesion using a minamo wire.
Crossing the 99% very calcified proximal left circumflex lesion proved challenging. However, we were able to cross it using Fielder XT.
Retroflexed LCX, anomalous long LM have high risk of stent dislodgment left main dissection and wire dislodgement.
The plan was to do double cush- however, no stent would go across the LCX lesion. We first pre dilated LM, LAD, LCX, ON lesions. We did encounter challenges in delivering balloons into LCX. After Predilation, we placed a stent in the OM and crushed it with a ballon placed in LM-LCX. However we faced extreme difficulty in placing stent in the LCX-LM. Finally, we had to take out both the OM and the LAD wire and were successful in delivering the stent across the LXC lesion using guideliner support (advancing the guideliner in to the LCX). After deploying the stent In the LM-LCX, we post dilated with an NC balloon.
We quickly crossed back into the the LAD – ie switched to a coullote technique..
Final angiograms demonstrated excellent stent expansion, no edge dissection and no geographic miss.
Impella was taken out at the end of the procedure and LFA was perclosed. Patient underwent PCI of RCA two days later and discharged home In great spirits
Extremely retroflexed LCX – showing that all stents started prolapsing- unable to deliver; Had to sacrifice LAD, OM wires to advance a guideliner into the LCX… and hence was able to place a stent into the LCX-LM. However this meant that we had to change to coullote technique; Placed a stent in the LAD – LM
Then simultaneous kissing balloon inflation of the LAD-LM-LCX
Talking JSKBT ( jailed semi inflated kissing balloon technique ) We did multiple JSKBTs here. Zameer our Pakistani fellow made these images.
Patient had CP/ NSTEMI in a decent sized town 100 miles away. Which has good sized hospital and interventional cardiologist’s and PCIs / primary etc are done. No CABG onsite. Cardiologist did angio for intervention purposes. Saw the anatomy Calcified distal left main, Ostial/ prox / mid LAD, 90% tight ramus, 90% bifurcation LCX/OM1 and CTO RCA. EF 30% with severe MR ( so even poorer forward flow / and overestimation of the LV function due to MR).
Referred to our surgeon. He said he can ! But very high risk. ( calcified aorta not. Great candidate to put on heart lung bypass / previous EVAR, Poor LV function, ) so referred to one of our colleagues – who said very high risk PCI. Referred back to surgery. Nothing happened. Meanwhile patient having symptoms. So the primary interventional cardiologist from the other city called us. Was going to need 3 to 4 wires with multiple balloons at a time. So needed an 8 French guide so did do single access Impella. Also deliberately took a short JL 3.5 guide ( which obviously has low support ) so we can sit outside this shortish left main and work
LAD was quite retroflex so you can appreciate flipping of hydrophilic coated wire with >120 bend with microcatheter assistance. Later changed to wiggle wire; So onwards LAD was started. Calcified, retroflex and quite some tortuous so IVUS was done after first run of 2.5 pre-dil; Still there was IVUS malfunction in mid autorun so predilated with 3.0 balloon and ReIVUS Heavy more than 270 degrees calcium is there; Further vessel preparation was done with 3.0 IVL all the way upto LMS
This is tight LCX and tight OM1. Kissing balloon inflations and then stent in LCX and JSKBT is OM. Notice 4 wires in there. Pretty good result. OM Latium looks really good. IVUD of LCX stent good. Did POT of the proximal LCX with NC balloon; This is the long 3.0 x 48 synergy xl. Extending from mid LAD to left main and have 3.0 x 15 balloons as JSKBTs in Intermediate and LCX
Couldn’t get the IVUS to distal edge to see if it is dissection or spasm. These new Hi Def boston IVUS shafts are flimsy and you push them and they get bent. Used three different catheters during this long intervention. Cuz it would get stuck in calcium and then either stop working or the shaft get bent. So images look like distal edge dissection. Placed a 2.5 mm shirt stent. Looked good after wards
IVUS from LAD stent back to left main. Had also done a 4.5 x 6 mm short NC balloon POT for left main. ( size mismatch between left main and LAD)
Of course without Impella. Wouldn’t have been able to do these. With occluded RCA and EF 30% with severe MR. I was getting flat line pressures with IVL and Thenleft main stenting with JSKBTs
By Dr. Arnav Kumar MD MSCR Interventional Cardiologist HCA Medical Center, Houston, Texas
Pt was 61 active pt – was sent from another hospital Late presentation STEMI The impella they had placed clotted his right leg. Then he had 23 min code for VFiB arrest – I placed LFA/LFV ECMO bedside. He had right leg ischemia from the prior placed impella. So I and vascular surgery switched to 5.5 impella via left subclavian. So only two options for pci access were either radial or stick the ECMO circuit. Angiogram with 100% LAD and LCX, 99% calcific LM. We preformed ivus guided bifurcation PCI of LM-LAD-LCX after rotational atherectomy of the LM – LAD. Also reconstructed the whole LAD. Was able to do all radial fortunately.
Challenge #1. Here is the baseline angio. The challenge here is wiring the mid LAD. The wire tip shape needed to cross it is different than the one needed to reach it. Our solution – a dual lumen catheter (Sasuke) in the mid LAD which allows us to secure the D2.
Challenge #2. We wired the D1 to secure it during provisional LAD stenting. There is plaque shift +/- thrombus which shuts down the D1 by the time we have treated the mid LAD. Luckily we still had the wire in place – so in goes the Sasuke again. We were able to guarantee that the wires did not end up behind the stent struts.
Challenge #3. We did a proximal POT, pulled the jailed wire, and passed it down the LAD. I did not want to keep working on the Fielder. Note the brief detour into D2. Alas, we ended up with a dissection! After this point the patient started vomiting and the ST were really deep. I felt that the 6 Fr guide was workkng against us. As you can see much of the LAD has shut down. Our solution – intubate, insert Impella, upsize to 7 Fr.
Challenge #4. Here is the groin angio through the 14 Fr Impella sheath. The leg will likely become ischemic during the case- so we put in a retrograde SFA sheath for future ‘external bypass’.
Challenge #5. Our first angio after Impella placement shows clot in the entire LAD!!! 😳😩 I called for Penumbra, but decided to make a pass with an Export while the cath lab was setting up. Surprisingly we were able to ‘uncork’ the LAD.
Challenge #6. The next step is to treat the D2 and optimize the mid LAD stent. There is stent recoil. IVUS showed a fibrotic lesion – we treated this with a cutting balloon and completed the LAD PCI. Or did we…
Challenge #7. The completion angio shows thrombus in the proximal LAD – address it with medications or aspirate? We tried PTCA but it embolized. Well, by this time the Penumbra was set up. We were able to complete the procedure (again!). This is the final coronary angio.
Challenge #8 (No more, I promise): How to keep the leg perfused while the Impella was in place? Here is a clip of the initial angio through the Impella sheath. The third clip is through the SFA sheath (using a micropuncture dilator) after the external bypass has been set up (right CFA -> left SFA). I do this to confirm pulsatility in the occluded leg.
This is what the set up looks like. There are several advantages to doing it this way. The retrograde sheath is easier to insert, doesn’t compromise antegrade flow to the leg, allows you to do an angio to confirm Impella sheath closure (if done), perform internal balloon tamponade on the proximal arteriotomy (if needed) and importantly – makes sure there is no dead zone in the CFA. As a bonus, you can close this with an AngioSeal later if needed.
The End. Question: How would you take out the antegrade sheath? Manual and balloon tamponade the CFA from contralateral? Answer: They are both retrograde. The angio shows it. It looks antegrade because of the body habitus. The typical sequence is: 1) Remove Impella 2) Exchange Impella sheath for new sheath without flushing 3) You may do an angio from the lower (SFA) sheath at this stage. This is optional. 4) Treat the proximal arteriotomy with Manta or double Perclose. 5) Confirm closure with injection through the lower sheath. 5a) Consider balloon tamponade from the lower sheath if needed. 6) Close the lower arteriotomy if the SFA is ‘clean’ – you must use a device. It is too deep for manual hemostasis. 7) Confirm close from the contralateral side.
1) These are recommendations for Impella inserted in an emergency – and expected to stay in for some time. Usually there is no time for Preclose if the patient is crashing. 2) Also, I don’t Preclose unless I know the Impella is coming out within 6-12 hours. 2b) We have left the sutures in longer but management becomes an issue if the CCU stay is prolonged. 3) You don’t have to put a new Impella sheath in. Any 14 Fr sheath will do. 4) The idea is that there may be thrombus in the old sheath – in the space between the sheath and the Impella. 4b) Of course, you can hook it up to pressure to keep it open – but we have had thrombus form despite that too. 5) When the Impella comes out, you can use your favorite method to obtain hemostasis. Double Perclose is just one. 6) Stick the SFA in the cleanest part – avoid being too close to the Impella sheath. You don’t want the lower sheath tip ‘tucked under’ the Impella sheath.
We have left Impellas in upto 5 days with good leg perfusion using this method. The best part is that you can take it out yourself in the cath lab. No need for the OR. Question: SA; trying to understand.. The need for# 6? Why is the SFA stick needed? This is required when the Impella sheath is occlusive in the iliacs or the CFA. In such cases the leg with the Impella becomes ischemic.
One way to prevent this is to gain antegrade access into the CFA or SFA and create an ‘external bypass’. Usually this is done with US guidance and is a little tricky.
Our method makes it wasy because you can stick the SFA without changing the side you are standing on. Also, if you use a roadmap (like we did) you can do it without US. Because there is usually some flow via the profunda: CIA -> IIA -> PFA -> CFA/SFA.
Question: Also, for the SFA are you using an Arrow sheath ? Answer: Yes, always an Arrow sheath. Given the depth of the vessel and the angles involved, you need a braided sheath. Non-braided sheaths will typically soften and kink.
Here is a case I recently presented at CVI. I broke it up into different videos for teaching. A PDF of the complete presentation is included at the end.
62 year old man with HTN, DM2, and CKD 3. Presents with progressive angina for three months. Now CCS class 3. The referring MD sent him for a CTA – no stress test available. How would you approach this?
There are several notable features:
Anonymous left main from the non-coronary cusp.
Proximal LAD occlusion with a diseased mid segment.
Bifurcation disease involving the high ramus/OM1.
Patent LIMA, which supplies the distal LAD. 4b. Patent intracostal branch from the LIMA, which may be causing a steel phenomenon.
Moderate disease involving the takeoff of the high PDA.
Occluded SVG to the PDA (not shown).
As such, it is difficult to determine the exact location of the ischemia. There is also a second diagonal branch, which is diffusely diseased and supplied by epicardial collaterals.
I asked the referring MD to get a stress test. The patient had ischemia in the basal and mid anterior wall and anterolateral segments. Our plan was to treat the high Ramus/OM1 and then proceed with the LAD CTO PCI. Here is the LCX PCI. We performed Culotte.
This is the dual injection angio for CTO PCI planning.
Here are some potential options for the CTO PCI. Antegrade contrast modulation seemed to be our best bet. Here is the sequence for this rather novel crossing technique…
Proximal cap puncture with Gaia 2
The modified Carlino injection. Note the three breakout stains. In chronological order, these are a diagonal, a septal, and the distal true lumen.
These are the three stains. Carlino has a name for this mechanism of CTO crossing. He calls it hydrodynamic contrast recanalization. Or HDR for short. This is a new term that you will be hearing about quite a bit in the future.
It can be difficult to tell if the ongoing stain is re-entry or infiltration into the extra plaque space. A retrograde injection clarifies this.
A Fielder XT without a tip bend is advanced across the channel made by the contrast under fluoroscopic guidance.
The micro catheter is an advanced over this wire. We confirm distal re-entry by means of pressure transduction and…
A distal tip injection.
Here is the final angiogram. This case highlights a new CTO crossing technique introduced by Mauro Carlino, and refined by us at UT. He calls it HDR as noted above. We have just submitted a paper describing the technique, and hopefully it will be accepted (soon!).
For our colleagues: CTO PCI is a mature field and several strategies for crossing CTOs have been developed. Most of them use wires. This ‘new’ technique is not so new – it is modification of an older technique which uses contrast injections. It is called Carlino after the interventionalist who described it.
By Amin H. Karim MD Parth Desai MD (Interventional Fellow)
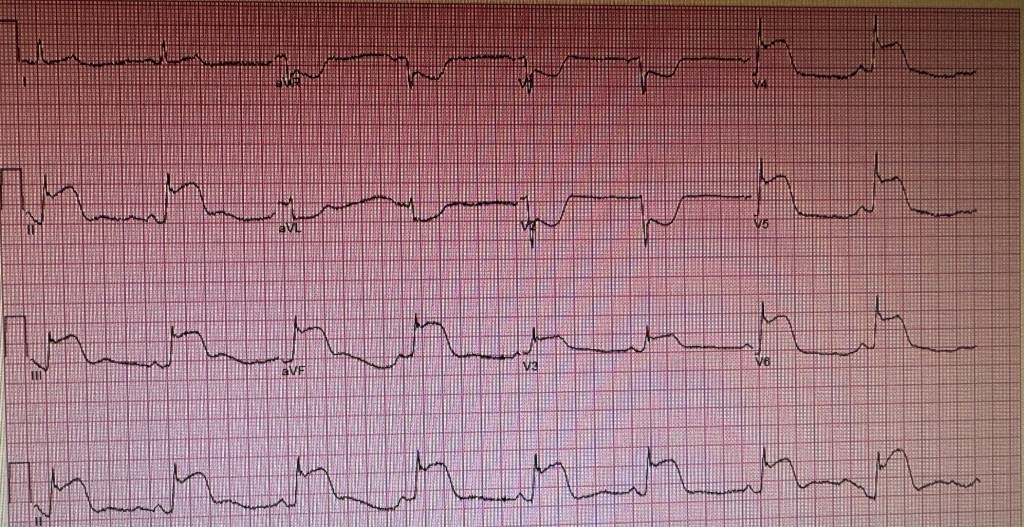
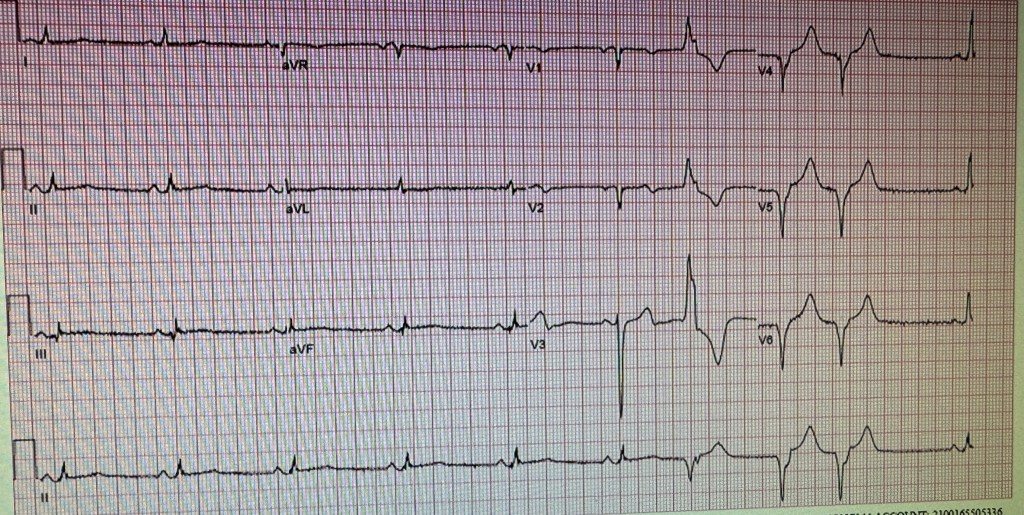
CASE REPORT: A 61 year old Caucasian female presented with sever chest pains for 3-4 hours. EKG was obtained.
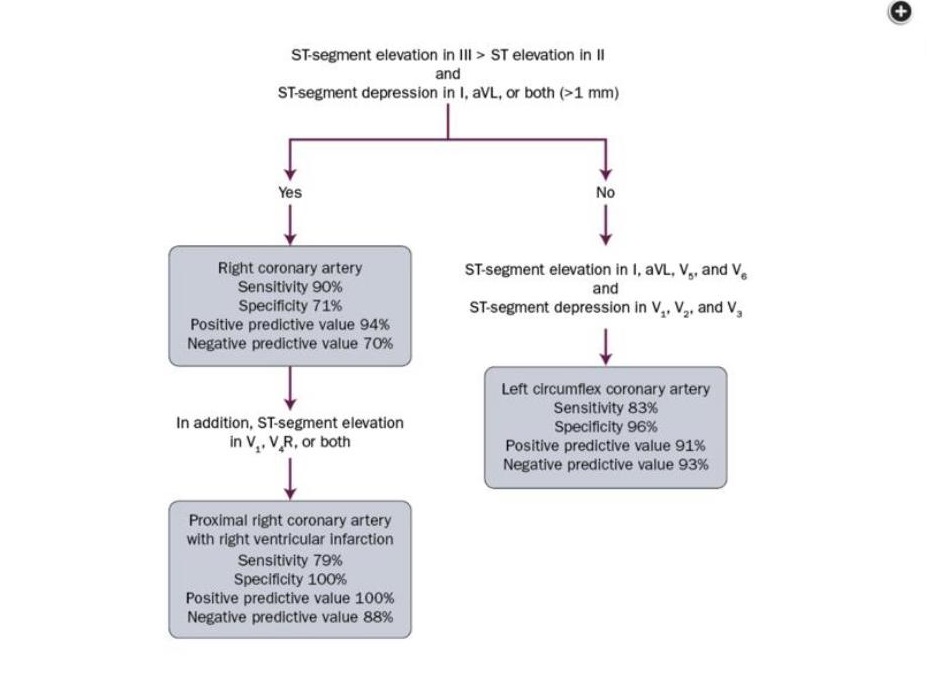
We put it through our panel to see if they could figure out the location of the culprit lesion in this STEMI patient. The answers ranged from a large dominant circumflex or RCA to a combined lesion in the LCX and LAD. Take a moment and see if you can tell the location of the lesion. Perhaps you can use the chart that was went by Dr. Syed Fazal:
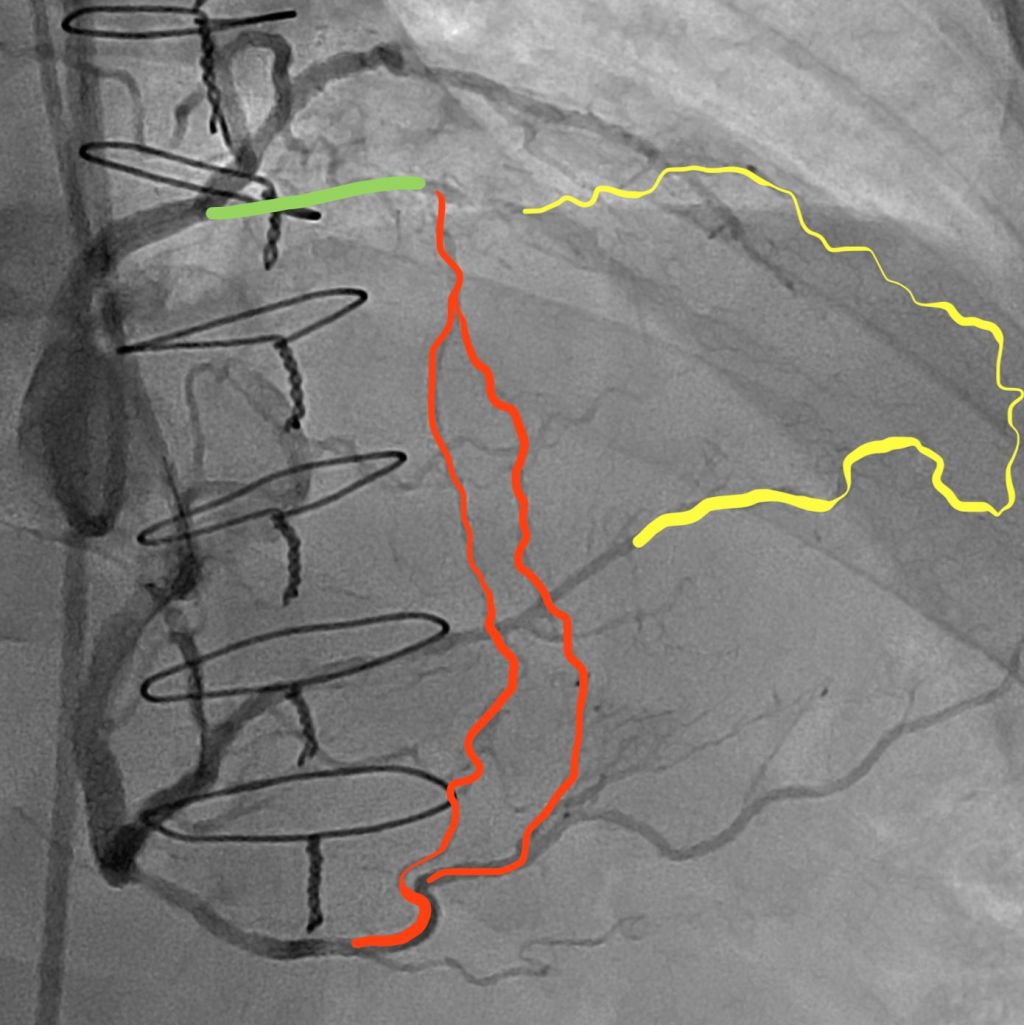
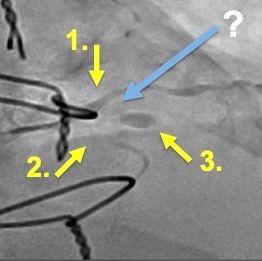
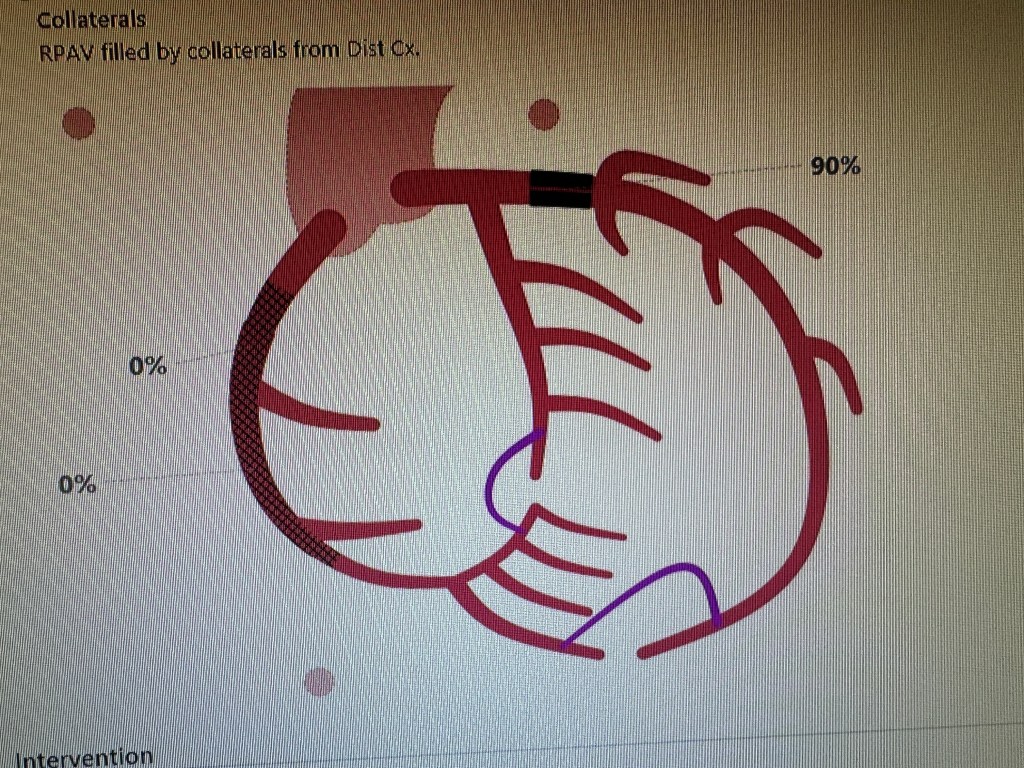
Cath showed the following:
A subtotal occlusion of the left circumflex coronary artery before the obtuse marginal takeoff. It does not look that this distal circumflex supplies the anterior wall or the apex of the left ventricle.
Here is the view of the LAD (Left anterior descending) coronary artery showing there is no obvious lesion or any cut off to suggest that there may have been a clot in the artery which would have caused the anterior wall changes in the EKG.
We crossed the LCX lesion using a whisper wire, pre dilated it and placed a 3×18 mm Synergy DES with a satisfactory result.
So the question remains, why the extensive changes on the EKG when the lesion is localized and one would have expected changes in the inferior or inferior and lateral leads. Could the patient have a hypercoagulable state? malignancy?. There is no evidence of spontaneous dissection. Concomitant spasm in the LAD with the thrombus in the LCX is a possibility (reported by us in 1990’s and the two published articles are on this website). her troponins peaked at 8500. Echocardiogram showed wall motion abnormalities as follows:
EKG done the next day. Patient did well clinically. The global ejection fraction was 45-49%. Incidentally patient also took Adderal of and on for attention deficit disorder. There are reports that these drugs can increase the incidence of cardiovascular events. INDEBTED TO COMMENTS ON THIS CASE BY: Prof. Salman Arain Dr. Syed Arman Raza Dr. Farhan Katchi Dr. Zubair Mohammad Syed Dr. Syed Fazal Dr. Usman Mustafa
A 85 year old dialysis patient who presented with non stemi last week; we stented his occluded RCA with good result and brought him back today for his LAD lesion; looked straightforward but the access to LM proved to be a challenge being on the roof of the sinus in a dilated aging aorta. The lesion itself looked juicy and inviting! 🙂 Iliac was tortuous so we ended up kinking a few catheters till we decided to beat it and go with the longest 7F sheath in the arsenal and a FR 3.5 came to our rescue. The rest was a piece of cake with predilatation and a Resolute Onyx Drug eluting stent 3.0 x 18 stent post dilated with 3.5 mm NC. According to Dr. Waqas Qureshi, MB guide would be another option in cases of wide aortic roots.
A 85 year old patient on hemodialysis, presented with acute coronary syndrome. Cath showed a totally occluded RCA. This is just a straight forward case being posted initially to test the website and ease of uploading videos.
Here is the left coronary showing a tight proximal LAD but not a culprit lesion.
View of left coronary showing a tihth proximal LAD lesion but not the culprit.
Anohter left coronary view showing collaterals to the RCA.
A large occluded RCA in the proximal portion with a possible clot.
RCA double sired with a High Torque Floppy wire and a Sion Black wire.
Lesion predilated and stent with a Synergy DES 4.5 x 28 mm stent and post dilated with a 5.0 x 15 non compliant baloon at nominal pressues. TIMI 3 flow achieved. Intracoronary nitroglycerin and intracoronary nitroprusside used. Patient remained stable throughout. Stent placement in the LAD is planned in 3 days.
👆🏼This is the case that almost got away. 58 year old man with a failed attempt by the referring MD. He has severe ischemia in the inferolateral region. He does not have LAD or left main disease, so not an upfront CABG candidate.
Tortuous RCA
Tortuous RCA
Here is the attempted intervention. The operator is experienced but does not do CTOs. He used an OTW balloon and some workhorse wires. He stopped because he was unable to cross and the patient started complaining of angina.
But before I do, let me just lay out some initial considerations:
Guide support
Crossing the tortuosity (or tortuosities!)
Prevention of spasm +/- accordion effect
Lesion prep – given the nodular calcium appearance.
I felt that a soft tipped hydrophilic wire was essential to start. Also, up front guide extension…
We used a Luge wire and a 6 Fr GuideLiner. Turns out, that this was the easiest part of the entire procedure. 😳 more to follow 👆🏼This is BAT. Balloon aided tracking. Very helpful for advancing guide extenders over long distances, when the path is relatively open. There is a 2 mm balloon, partially extending out of the GL tip. It is inflated to 4 atm. Both balloon and GL are advanced together. This is not my attempt. But my commentary is that the operator has good support but his choice of a microcatheter (MC) could have been better. Braided MCs perform better than OTW balloons and unbraided MCs. Also, the wire should ideally be a highly torquable wire with an appropriate tip. Most workhorse wires don’t have adequate support and/or the appropriate tip – hydrophilic tapered would be ideal.
This is our first attempt – we used multiple wires and tip shapes. Fielder XT, Sion Black, Fighter, and Gladius Mongo.You can see that I am using the Luge as a marker wire. I also have a dual lumen catheter so that the wires don’t interact (with the bonus advantage of support).
Anyway, in the interest of time and not to bore the audience with the drawn out style (which is how I teach!), we decided to take another hi-res view of the lesion. Turns out it is very complex because it comes off in a retroflexed manner, there plaque proximal to it which deflects the MC, and there is a hinge point which makes the lesion even tighter in systole!!! I have deliberately slowed it down here. So, last question. What do you do here? How to solve this twist in the tail?!
What we ended up doing (with luck as much as intention) is creating a ‘biplanar curve’ aka a spiral tip. It bent both downwards and to the side. This allowed us to ‘cork screw’ the wire (Mongo) into the PDA.
But, to put it in perspective, what looks like an obvious solution (now) took years of doing complex cases to achieve. And hundreds if not thousands of cases
Final thoughts. There are three ways to use a balloon to advance a GL.
Anchoring. Best for short distances with few bends. You can do it repeatedly as you go down the vessel.
Inch worming. This is where you deflate the balloon and advance the GL over it. Best for heavily calcified arteries and/or tracking within stents.
BAT. Best for arteries with extreme tortuosity, which are otherwise patent proximately. Or to go down open grafts.
Thank you but we tried all combinations I could think of. With all types of wire tips. Even a Carlino to make a channel and a knuckle. Nothing worked – primarily because the lesion is foreshortened in our initial working view and because the ‘hinge’ at the PDA origin changes the orientation of the opening with every heart beat. A dynamic stenosis! BTW, the wires we used included a Fielder XT, Fighter, Mongo, Sion Black, and a Gaia 2. The bi-planar tip is on the Mongo. And not with the usual curve added to the pre-shaped tip. Only after we gave it a sideways second curve. You can see it unfold a bit, before we were able to advance it across the stenosis.
Prof. Salman Arain
Permission to reproduce above obtained from Dr. Salman Arain on Nov 27 2023