By Amin H. Karim MD
Joseph Aaon MD (Interventional fellow)
We present a case of acute myocardial infarction with total occlusion of the left anterior descending coronary artery. A 85 year old male presented with several hours of atypical chest pain. EKG at a free standing ER showed ST elevation in the antero-septal leads. Catheterization was done in the 90 minute door to balloon time and showed the following: There was a vessel alongside of the left anterior descending coronary that looked like a bridging collateral. Our question was: is this a chronic occlusion with a collateral or was it an acute occlusion causing the chest pain and EKG changes. Orthogonal views were obtained to make sure we do not end up wiring the bridging collateral, which may give the impression of wiring the true lumen. hence it may not hurt to obtain one or more orthogonal views to confirm the position of the wire. The micro catheter also helps if there is confusion. Injection of the contrast into the vessel can differentiate a bridging collateral from a branch of the vessel.
The lesion was crossed using a micro catheter and a whisper wire. 3.5 x 38 mm DES was placed. Final result was satisfactory.
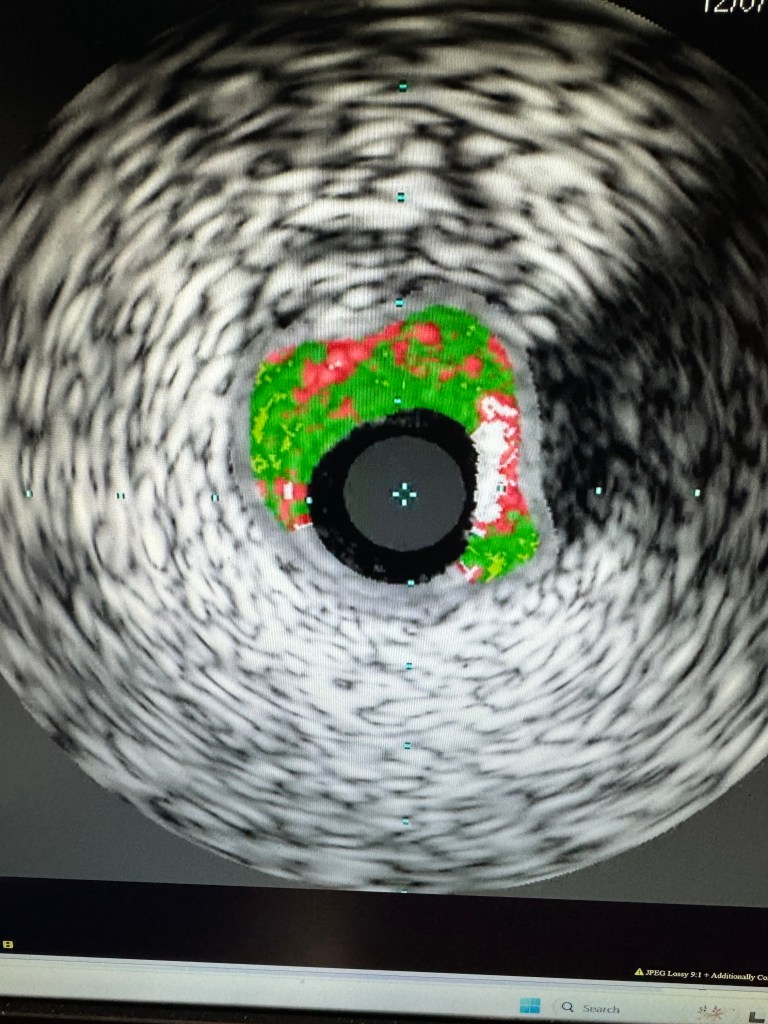
IVUS pre dilatation showed a fair amount of calcium.
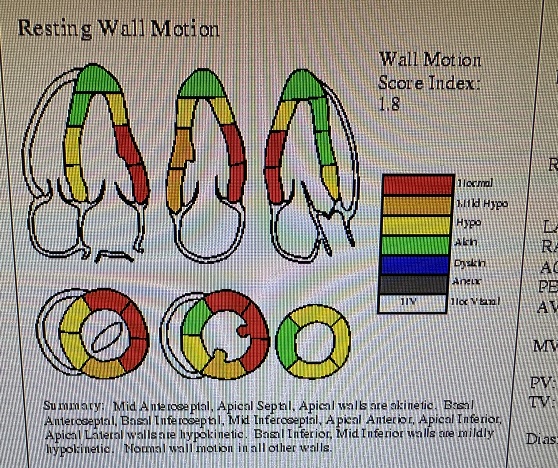
Echocardiogram obtained the next day showed anterior wall and apical akinesis. There was a layered thrombus in the apex of the left ventricle. Patient was anticoagulated with warfarin, in addition to clopidogrel and aspirin. Plan was to discontinue aspirin in 2 weeks to reduce the risk of bleeding.