A CASE OF POSTOPERATIVE COMPLICATION OF SURGICAL MITRAL VALVE REPLACEMENT.
Amin H. Karim MD
CASE: A 71 year olf Caucasian male with history of hypertension and hyperlipidemia, and chronic atrial fibrillation, developed non-rheumatic mitral valve regurgitation secondary to mitral valve prolapse, which had gradually progressed over a decade years to severe regurgitation, accompanied by moderately severe tricuspid regurgitation. Patient tolerated the valvular lesions for many years till he became symptomatic with NYHA Class III dyspnea and agreed for intervention.
CARDIAC MRI: In November 2024, cardiac MRI revealed bi-leaflet mitral valve prolapse, with severe left atrial enlargement and moderate tricuspid regurgitation. The global ejection fraction was 65% with biventricular dilatation, and basal and mid inferolateral wall scarring. Mitral and tricuspid annulus were dilated.
TWO DIMENSIONAL ECHOCARDIOGRAM: On Echocardiogram, right ventricular function was low normal. Left ventricular ejection fraction was normal. There was mitral valve prolapse due to myxomatous degeneration, severe mitral regurgitation with regurgitation fraction of 51% and estimated regurgitant volume of 56 ml. Pulmonary artery pressures were normal. Cardiac catheterization showed normal coronaries
With a low BMI and good overall health, he was felt by the cardiovascular surgeon to be low risk for surgery and MitraClip therefore not warranted.
MITRAL VALVE REPAIR SURGERY: Mitral valve repair with a 34 mm physio 2 flexible annuloplasty ring; Intra-aortic balloon pump; Tricuspid valve repair with a 28 mm triad rigid ring; Biatrial maze utilizing the encompass clamp, RF clamp and cryoprobe; Left atrial appendage ligation with a 45 mm atrial cure mini atrial clip:
Following mitral valve repair there was no mitral regurgitation with a long segment of coaptation beneath the annular plane. The transmitral gradient was 1 mm Hg. Similarly following tricuspid valve repair there was no regurgitation with the trans tricuspid valve gradient of 1 mm. Following bi-atrial maze procedure, the patient converted to sinus rhythm. However, when the cardio pulmonary bypass was reversed and the patient was being closed, he went to ventricular fibrillation followed by defibrillation. Frequent PVCs were observed. Intravenous amiodarone and magnesium were started; His blood pressure started to drop and vasopressors were increased and intra-aortic balloon placed. His hemodynamics improved and was watched in the OR with echo. There was inferior wall hypokinesis. He was maintained on low dose dobutamine, vasopressin and norepinephrine. His global ejection fraction was reasonable; chest was closed, but before he could be transferred out of OR he developed ventricular fibrillation again. His chest was opened and direct cardiac massage and cardioversion done with return of circulation. ECMO (Extracorporeal Membrane Oxygenation) was initiated. He was transferred to the cardiac cath lab and underwent emergency coronary angiography.
CORONARY INTERVENTION: Coronary angiography showed the dominant left circumflex was occluded in the mid potion.
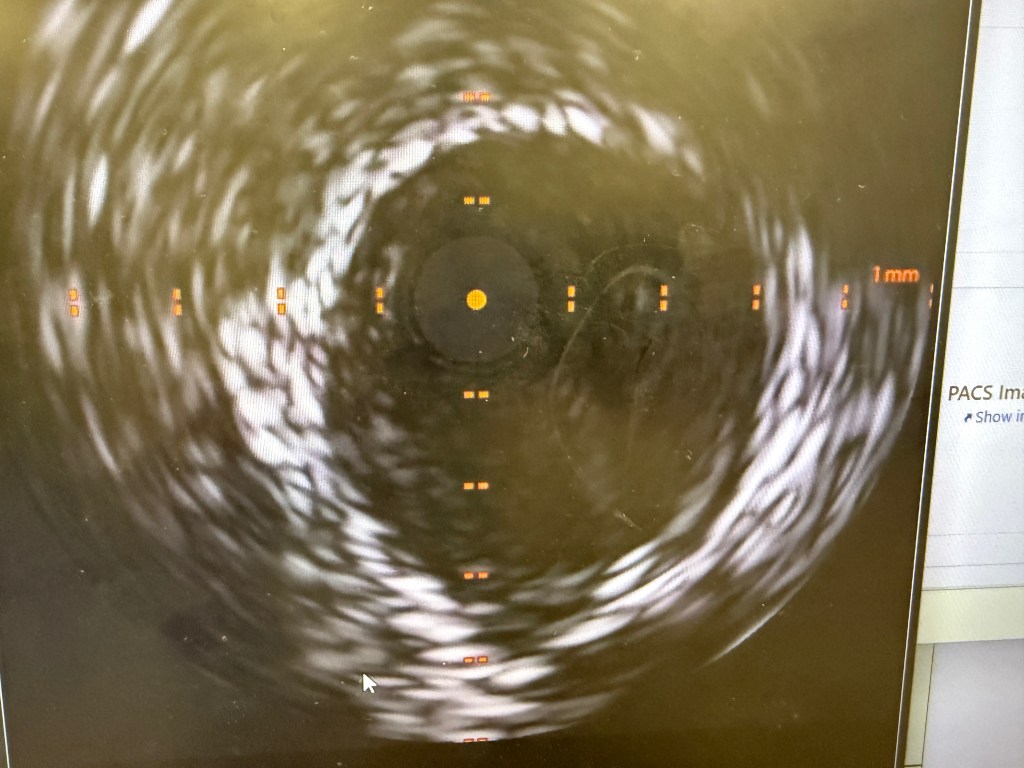
IVUS showed possible edema around the left circumflex and it was felt that the circumflex was occluded due to pressure from the mitral valve ring. Stent was placed with recanalization. Impella was placed in the cath lab and the intra-aortic balloon was removed.
Intavascular Ultrasound (IVUS) shows the edema/hematoma? aeound the left vircumflex artery.
A 3.5 mm x 32 mm Synergy drug eluting stent was placed in the mid circumflex coronary artery with a good result. The intra-aortic balloon was removed.
INTENSIVE CARE UNIT: Patient remained with supported blood pressure, with severe anemia needing multiple blood transfusions. Transesophageal echo showed severely depressed right and left ventricular systolic function. Patient was taken back to O.R. for exploration and washout. On return to ICU noted to have ST elevation in lead VII. Taken back to cath lab and coronary angiography done showing that the circumflex stent was patent.
FOLLOWUP: 10 days after mitral and tricuspid valve repair and coronary intervention, patient is off ECMO, and on Impella support. He is awake but does not follow commands. His global ejection fraction on echocardiogram is mildly depressed (40-45%) with trace of mitral and tricuspid regurgitation.
Sarai Anayansi Zárate Chávez Universidad Anáhuac campus Oaxaca
Juan Pablo García Guzmán Universidad Anáhuac Mexico campus Norte
Amin H. Karim MD Institute of Academic Medicine, Houston, Texas Weill Medical College of Cornell University.
What Is a Blood Clot? A blood clot also referred to as a thrombus (plural: thrombi), intravascular clot, or coagulum is a gelatinous or semi-solid mass of coagulated blood that forms within the circulatory system. When such a clot develops in the deep venous system, most commonly in the lower limbs, it is termed deep vein thrombosis (DVT), although it can also occur in the upper extremities. A major complication of DVT is embolization, in which one or more thrombi detach and travel through the venous circulation often originating in the legs, pelvis, or groin and reach the pulmonary arteries, leading to a pulmonary embolism (PE). This condition can be life-threatening and requires immediate medical intervention. Thrombus Formation and Intracardiac Clot Dynamics A thrombus also referred to as a clot, blood clot, embolus (when mobile), or thromboembolus (when causing obstruction) is the result of a complex interaction between endothelial injury, abnormal blood flow (stasis or turbulence), and a hypercoagulable state, often summarized by Virchow’s triad. In the setting of acute vascular injury, particularly in acute coronary syndrome (ACS), clot formation begins with platelet adhesion to exposed subendothelial proteins at sites of plaque rupture or erosion. Once adhered, platelets become activated, change shape, and release a variety of pro-thrombotic substances including thromboxane A2, ADP, and serotonin, promoting further platelet activation and local vasoconstriction. The surface expression of glycoprotein IIb/IIIa receptors increases, facilitating platelet aggregation through fibrinogen bridging. Concurrently, the coagulation cascade is triggered, leading to thrombin generation. Thrombin amplifies platelet activation and converts fibrinogen into fibrin, which stabilizes the growing thrombus. As fibrin is laid down, a stable platelet-fibrin thrombus forms, which may partially or completely obstruct the vessel. If embolized, fragments of the thrombus may lodge downstream, causing ischemia or infarction. Intracardiac thrombi form under somewhat different circumstances, often related to blood stasis or structural heart disease. In the left ventricle, thrombi can arise after anterior myocardial infarction, especially with regional wall motion abnormalities such as apical akinesis or dyskinesis. In non-ischemic dilated cardiomyopathy, the risk is lower but still present, particularly when left ventricular ejection fraction is severely reduced. The left atrium, particularly the left atrial appendage, is a common site for thrombus formation in patients with atrial fibrillation, atrial flutter, or significant mitral valve disease. Even in sinus rhythm, atrial mechanical dysfunction—as in cardiac amyloidosis—can predispose to thrombus formation. On the right side of the heart, thrombi may form in cases of central venous catheters, intracardiac devices, severe right ventricular dysfunction, or hypercoagulable states. Additionally, mechanical prosthetic valves, especially with inadequate anticoagulation, are a high-risk source of thrombus formation and systemic embolism. Paradoxical embolism can occur in the presence of a patent foramen ovale (PFO) or atrial septal defect (ASD), where venous thrombi bypass the pulmonary circulation and enter the systemic arterial system through a right-to-left intracardiac shunt.
Diagnosis: Tests The main diagnostic tests for detecting thrombi in the left ventricle are transthoracic echocardiography (TTE) and cardiac magnetic resonance imaging (CMRI) with delayed gadolinium enhancement. TTE is the most used initial technique due to its availability and low cost: however, its sensitivity is limited (approximately 21-35%), although its specificity is high (95-98%). The use of intravenous contrast agents in TTE improves sensitivity (up to 64%) without losing specificity. Transthoracic echocardiography has been utilized for identifying left ventricular thrombi since the early 1980s. In recent years, the introduction of echocardiographic contrast agents has improved detections accuracy, particularly in patients with suboptimal acoustic windows. TTE remains the initial diagnostic modality of choice for evaluating left ventricular thrombus. However, its limitations such as difficulty imaging patients with poor acoustic windows, can lead to considerable interobserver variability, potentially compromising diagnostic reliability. Cardiac magnetic resonance offers a diagnostic edge over echocardiography by allowing both myocardial tissue characterization and dynamic imaging. With recent advancements in imaging sequences and the use of paramagnetic contrast agents to enhance blood pool visualization, late gadolinium enhancement CMR may offer superior sensitivity for detecting left ventricular thrombi. Recent epidemiologic tests have provided that the incidence of left ventricular thrombus, using optimal imaging modalities, can reach up to 15% in patients with ST segment elevation myocardial infarction and up to 25% in those with anterior myocardial infarction. Although a standard transthoracic echocardiogram is frequently used for initial screening, its low sensitivity in detecting left ventricular thrombus requires the use of contrast (when not contraindicated) and/or cardiac MRI when there is a high pretest probability. Transesophageal echocardiography does not provide advantages for visualizing the ventricular apex and is not recommended as a second-line method for ventricular thrombi. The first study that was able to compare the diagnostic accuracies of CMRI, contrast TTE and noncontrast TTE was performed by Weinsaft et al. That demonstrated that even with administration of echocardiographic contrast agents, CMRI was still considerably more accurate modality in terms of thrombus detection. CMR with late gadolinium enhancement is the gold standard, with a sensitivity of 82-88% and specificity of 99-100%, as it allows differentiation of the thrombus (avascular without enhancement) from the surrounding myocardium. It is especially recommended when TTE (even with contrast) is not diagnostic or clinical suspicion persists. Cardiac computed tomography can incidentally detect thrombi, but it is not validated for this purpose Precise detection of left ventricular thrombi is crucial, as it frequently guides the initiation of anticoagulation therapy to reduce the risk of embolic complications. While current guidelines suggest that starting anticoagulation may be reasonable in patients with strong suspicion of thrombus such as those with apical akinesis or dyskinesis even without visible thrombus, selecting the most appropriate imaging modality is essential to ensure timely and evidence-based therapeutic decisions.
Complications The main complications of thrombi in the left ventricle are systemic embolic events, especially ischemic stroke and peripheral arterial embolisms. Embolization occurs because the thrombus can detach and migrate into systemic circulation, affecting organs such as the brain, kidneys, spleen, or extremities. The risk of embolization is particularly high in the first few weeks after an acute myocardial infarction and can reach up to 22% depending on the morphology and follow up of the thrombus. The incidence of systemic embolic events in patients with left ventricular thrombi varies depending on the population and clinical context. In patients with acute myocardial infarction (AMI), the incidence of left ventricular thrombus is 3.5% to 7.1% after previous AMI when cardiac magnetic resonance imaging is used, and the incidence of systemic embolism (including stroke) in the presence of thrombus is between 7% and 16% in the first few years after the event, with an annualized risk of 3.7% compared to 0.8% in patients without left ventricular thrombus. Other relevant complications include major adverse cardiovascular events (MACE), which include death, reinfarction, and hospitalization for heart failure. The presence of left ventricular thrombus is associated with a significant increase in mortality and long-term adverse cardiovascular events. In addition, patients with persistent thrombus are at increased risk of bleeding, especially if they require prolonged anticoagulation. The American Heart Association emphasizes that complete thrombus resolution is associated with lower mortality, while thrombus persistence, especially if mural and organized, carries a lower but not zero risk of embolization. The patient groups with the highest incidence of complications associated with thrombi in the left ventricle are mainly those with extensive acute myocardial infarction (AMI), especially anterior AMI, patients with ventricular aneurysm, and those with reduced left ventricular ejection fraction (LVEF). In addition, patients with dilated cardiomyopathy, either ischemic or non-ischemic, particularly those with severe systolic dysfunction, also have an elevated risk of embolic complications and major cardiovascular events. In the context of non-ischemic cardiomyopathy, patients with dilated cardiomyopathy show an even higher risk of systemic embolism compared to other non-ischemic etiologies and ischemic heart disease. The presence of mobile or protruding thrombi increases the risk of embolization, while thrombus persistence is associated with higher mortality and adverse events. The American Heart Association points out that the combination of anterior AMI, low LVEF, ventricular aneurysm, and delayed reperfusion are factors that identify patients at higher risk of embolic complications and mortality associated with thrombi in the left ventricle. The factors that increase the risk of thrombus formation in the left ventricle vary depending on the patient group, but they share pathophysiological mechanisms based on Virchow’s triad: ventricular dysfunction (stasis), endocardial damage, and inflammation/hypercoagulability. In patients with extensive acute myocardial infarction (AMI), especially anterior AMI, the highest risk factors are anterior location of the infarction, presence of ventricular aneurysm, left ventricular ejection fraction (LVEF) <30-40%, larger infarction size (elevated troponins), delayed reperfusion, and suboptimal coronary flow after intervention. The combination of reduced LVEF and segmental dysfunction (particularly apical) is the main predictor of thrombus and embolic complications or major cardiovascular events in all these groups. Systemic inflammation (elevated CRP) and the use of certain antithrombotic drugs may also contribute
Managment Management of left Heart Thrombi (RHT) The cornrstone of managment for intracardiac thrombus, particularly left ventricular thrombus, is therapeutic anticoagulantion. This strategy aims to reduce the risk of systemic embolism and promote trhombus resolution. Anticoagulation should be initiated promptly upon diagnosis, typically with intravenous unfractionated heparin, low molecular weight heparin, or a direct oral anticoagulant (DOAC). Transition to oral therapy with either warfarin or a DOAC is the recommended available evidence suggests that anticoagulation significantly lowers embolic risk and increases the likelihood of thrombus resolution compared to no or subtherapeutic treatment. In particular, a higher time in therapeutic range with warfarin is associated with superior outcomes and appears to outweigh the bleeding risks, even in the presence of concurrent antiplatelet therapy. The standard duration of anticoagulation is a minimum of three months.
Follow-up cardiac imaging, ideally using the same modality employed at diagnosis, should be performed at that point to assess thrombus resolution. If the thrombus persists without notable change, anticoagulation should be continued with periodic reassessment. In cases where the thrombus has decreased in size or displays features consistent with chronicity and reduced embolic potential, the decision to continue therapy should be based on ongoing embolic risk, such as persistent left ventricular dysfunction, aneurysm formation, or spontaneous echocardiographic contrast. If both the thrombus and contributing risk factors have resolved, evidenced by normalization of systolic function and absence of additional indications for anticoagulation, discontinuation of therapy may be appropriate. For patients who develop LVT in the context of prior MI (≥3 months) or chronic ischemic cardiomyopathy, no randomized controlled data exist to guide treatment duration. Nonetheless, anticoagulation for a period of 3 to 6 months is generally recommended. Beyond that, extended or indefinite therapy should be considered on a case-by-case basis, incorporating individual thrombotic and bleeding risks, recovery of ventricular function, and patient preferences through shared decision- making.
Management of Right Heart Thrombi (RHT) Right heart thrombi (RHT) are rare but potentially life-threatening findings, often associated with pulmonary embolism (PE) and right ventricular dysfunction. The management of RHT remains a clinical challenge due to the lack of randomized controlled trials and standardized treatment guidelines. However, observational studies and registry data suggest that anticoagulation alone is often insufficient, especially in cases involving mobile or serpiginous thrombi with high embolic potential. Initial management typically includes systemic anticoagulation with intravenous unfractionated heparin or low molecular weight heparin. This serves as a bridge to definitive therapy and may be appropriate in hemodynamically stable patients with non-mobile thrombi or contraindications to more aggressive interventions. For patients with mobile RHT or hemodynamic compromise, reperfusion strategies are generally preferred. Systemic thrombolysis has demonstrated lower mortality rates compared to anticoagulation alone, but carries a notable risk of major bleeding, including intracranial hemorrhage. Surgical embolectomy is another option, particularly in patients with contraindications to thrombolysis or when thrombi are large, organized, or entangled in cardiac structures. Catheter-directed therapies, including percutaneous aspiration thrombectomy (e.g., AngioVac, FlowTriever, AlphaVac), have gained attention as minimally invasive alternatives. These techniques allow for rapid thrombus removal with high success rates and a lower bleeding profile compared to systemic thrombolysis. Early outcomes are promising, although data remain limited and long-term efficacy has not been firmly established. Ultimately, the choice of therapy should be guided by thrombus characteristics (size, mobility, morphology), patient stability, comorbidities, bleeding risk, and institutional expertise. In general, mobile RHTs or those associated with acute PE warrant urgent intervention beyond anticoagulation alone. Multidisciplinary decision making often involving cardiology, critical care, interventional radiology, and cardiothoracic surgery is essential for optimizing outcomes.
Prevention Intracardiac thrombus formation is a recognized complication in patients with heart failure and reduced ejection fraction, particularly in those with non-ischemic dilated cardiomyopathy (DCM). Although left ventricular (LV) thrombi are more frequently documented, thrombi may also develop in the right heart chambers, especially in the presence of right-sided dysfunction, central venous catheters, cardiac devices, or systemic hypercoagulable states. The use of antithrombotic therapy for primary prevention of thrombus formation in this population remains a subject of ongoing clinical judgment. In patients with DCM who are in sinus rhythm and without prior thromboembolic events, neither aspirin nor warfarin has consistently demonstrated clear benefit in preventing thrombus formation or reducing major adverse cardiovascular events. Therefore, routine prophylactic use of these agents is generally not recommended. However, individualized assessment is essential, especially when additional risk factors such as atrial fibrillation, prior embolic events, severely reduced ejection fraction, or left ventricular aneurysms are present. In select subtypes of DCM that carry a higher inherent risk of intracardiac thrombus such as Takotsubo syndrome with apical ballooning, left ventricular noncompaction, peripartum cardiomyopathy, eosinophilic myocarditis, and infiltrative diseases like cardiac amyloidosis the use of oral anticoagulants (e.g., warfarin) or parenteral agents may be considered on a case-by-case basis. In contrast, low-dose aspirin may offer some theoretical antiplatelet benefit, but its role in thrombus prevention remains less defined. Long-term anticoagulation may be appropriate for patients with persistent ventricular dysfunction or recurrent thromboembolic risk, provided the bleeding risk is acceptable.
Bibliografia link Mathevosian, S., & Ranade, M. (2022). Right Heart Clot-in-Transit: Endovascular Therapies. Seminars in interventional radiology, 39(5), 515–522. https://doi.org/10.1055/s-0042-1757942 Sakellariou, X. M., Efstathopoulos, A., Stamatis, K. V., Nikas, D. N., & Kolettis, T. M. (2020). Treatment of Mobile Right Heart Thrombi. European journal of case reports in internal medicine, 7(12), 001918. https://doi.org/10.12890/2020_001918 Patel, A. N., Amrutiya, R. J., Manvar, B. N., & Patel, A. (2022). A proposed approach for the management of clot-in-transit. Cureus, 14(8). Lawrence LK Leung, M. D. (2025). Overview of hemostasis. https://shorturl.at/hkxsH Levine, G. N., McEvoy, J. W., Fang, J. C., Ibeh, C., McCarthy, C. P., Misra, A., Shah, Z. I., Shenoy, C., Spinler, S. A., Vallurupalli, S., Lip, G. Y. H., on behalf of the American Heart Association Council on Clinical Cardiology, Council on Cardiovascular and Stroke Nursing, & and, S. C. (2022). Management of patients at risk for and with left ventricular thrombus: A scientific statement from the american heart association. Circulation, 146(15), e205–e223. 10.1161/CIR.0000000000001092 Warren J Manning, M. D. (2024). Echocardiography in detection of cardiac and aortic sources of systemic embolism. https://shorturl.at/mR7gN Watson, N. W., Weinberg, I., Dicks, A. B., Carroll, B. J., & Secemsky, E. A. (2024). Clinical outcomes and predictors of advanced therapy for the management of right heart thrombus. Circulation: Cardiovascular Interventions, 17(4), e013637. 10.1161/CIRCINTERVENTIONS.123.013637
Wilson S Colucci, M. D., & Gregory YH Lip, MD, FRCPE, FESC, FACC. (2025). Left ventricular thrombus. https://shorturl.at/Zf9oO Kleindorfer, D. O., Towfighi, A., Chaturvedi, S., Cockroft, K. M., Gutierrez, J., Lombardi-Hill, D., Kamel, H., Kernan, W. N., Kittner, S. J., Leira, E. C., Lennon, O., Meschia, J. F., Nguyen, T. N., Pollak, P. M., Santangeli, P., Sharrief, A. Z., Smith, S. C., Jr, Turan, T. N., & Williams, L. S. (2021). 2021 guideline for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline from the American heart association/American stroke association. Stroke; a Journal of Cerebral Circulation, 52(7), e364–e467. https://doi.org/10.1161/STR.0000000000000375 Levine, G. N., McEvoy, J. W., Fang, J. C., Ibeh, C., McCarthy, C. P., Misra, A., Shah, Z. I., Shenoy, C., Spinler, S. A., Vallurupalli, S., Lip, G. Y. H., & American Heart Association Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; and Stroke Council. (2022). Management of patients at risk for and with left ventricular thrombus: A scientific statement from the American Heart Association. Circulation, 146(15), e205–e223. https://doi.org/10.1161/CIR.0000000000001092 Camaj, A., Fuster, V., Giustino, G., Bienstock, S. W., Sternheim, D., Mehran, R., Dangas, G. D., Kini, A., Sharma, S. K., Halperin, J., Dweck, M. R., & Goldman, M. E. (2022). Left ventricular thrombus following acute myocardial infarction: JACC state-of-the-art review. Journal of the American College of Cardiology, 79(10), 1010–1022. https://doi.org/10.1016/j.jacc.2022.01.011
Sharma, N. D., McCullough, P. A., Philbin, E. F., & Weaver, W. D. (2000). Left ventricular thrombus and subsequent thromboembolism in patients with severe systolic dysfunction. Chest, 117(2), 314–320. https://doi.org/10.1378/chest.117.2.314 Ram, P., Shah, M., Sirinvaravong, N., Lo, K. B., Patil, S., Patel, B., Tripathi, B., Garg, L., & Figueredo, V. (2018). Left ventricular thrombosis in acute anterior myocardial infarction: Evaluation of hospital mortality, thromboembolism, and bleeding. Clinical Cardiology, 41(10), 1289–1296. https://doi.org/10.1002/clc.23039 Albaeni, A., Chatila, K., Beydoun, H. A., Beydoun, M. A., Morsy, M., & Khalife, W. I. (2020). In-hospital left ventricular thrombus following ST-elevation myocardial infarction. International Journal of Cardiology, 299, 1–6. https://doi.org/10.1016/j.ijcard.2019.07.070
Amin H. Karim MD Institute for Academic Medicine Houston, Texas
Today a 65 year old patient showed up in the office. He had not seen me for last 5 years for whatever reason and now needed a surgical clearance. He worked as a RN at a Houston Hospital and subsequently at the VA Hospital;
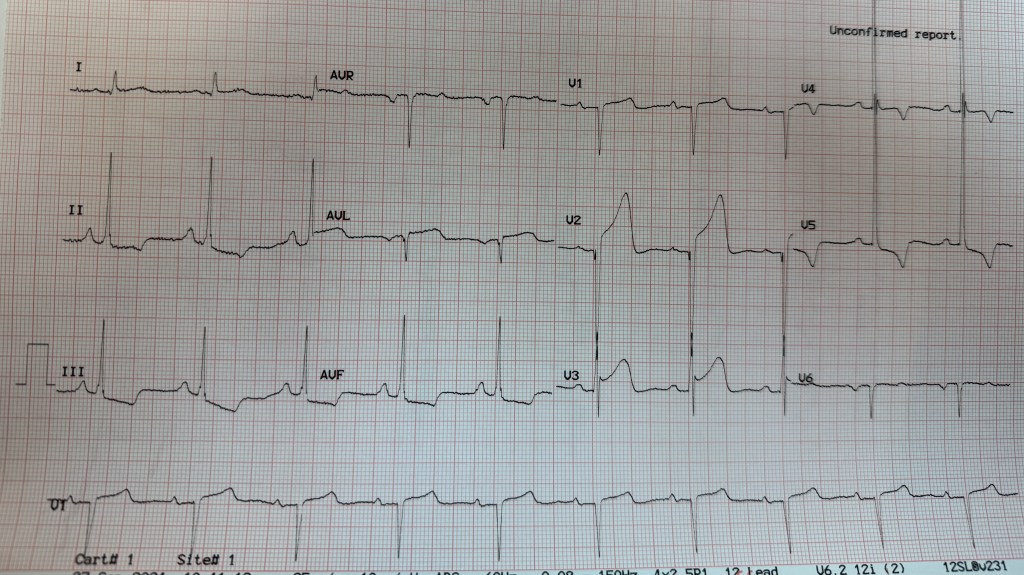
I did a routine EKG as follows:
It was unchanged from his previous EKGs from years ago. When he was following with me, he had a cardiac workup including imaging tests showing normal coronaries.
On taking his interval history, I found some interesting facts. While working at the VA he had some atypical chest pain. He went to the ER and had an EKG and was seen by a cardiologist stat. He was rushed to the catheterization lab and had a diagnostic cardiac catheterization which showed normal coronaries. A few months later he had similar chest pain and again went to the ER at a premier hospital in town for evaluation. An EKG was done and STEMI was called immediately. He protested to the cardiologist that he had cardiac catheterization a few months ago and that it was normal! The cardiologist was insistent that he have another one since his EKG showed that he was having a heart attack and could die. His protests were to no avail and he was rushed to the lab and had another diagnostic cardiac study which of course showed normal coronaries. The cardiologist came and apologised to him for not listening to him.
Now it was my turn to beat him on the head and tell him: ” You have STEMI written on your forehead. Wherever, you go you will be treated with emergency response and the STEMI will be summoned and you will be rushed in an elevator with a security guard holding it! Once in the cath lab you will be surrounded by a frantic team counting minutes!
So this is what you are going to do. You will take a copy of your EKG, go to Office Depot and have it reduced and laminated; then carry it with you in your wallet and if you land in the ER and before they wheel you away to the cath lab, show them the EKG and tell them that your EKG is always abnormal and that they should compare to see if there are any changes. Otherwise you will someday end up with a clot in your hand or leg or some other complication!
I think he got the message.
No offence meant and take it in the lighter vein, but I am sure every interventional cardiologist taking emergency calls faces these alarms and the 90 minutes door to balloon time does not allow much margin to hunt for old EKGs!