
By Dr. Salman Arain MD
Here is a case I recently presented at CVI. I broke it up into different videos for teaching. A PDF of the complete presentation is included at the end.
62 year old man with HTN, DM2, and CKD 3. Presents with progressive angina for three months. Now CCS class 3. The referring MD sent him for a CTA – no stress test available. How would you approach this?
There are several notable features:
- Anonymous left main from the non-coronary cusp.
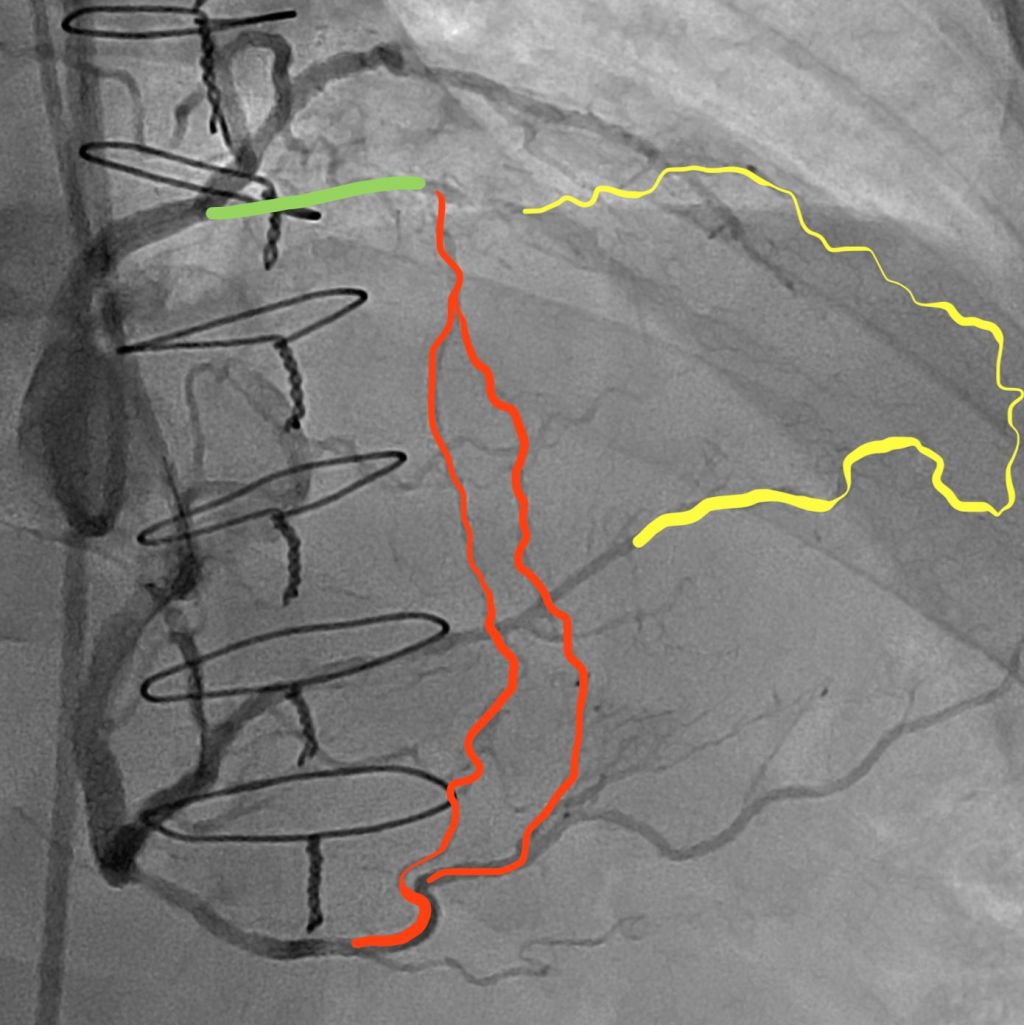
- Proximal LAD occlusion with a diseased mid segment.
- Bifurcation disease involving the high ramus/OM1.
- Patent LIMA, which supplies the distal LAD.
4b. Patent intracostal branch from the LIMA, which may be causing a steel phenomenon. - Moderate disease involving the takeoff of the high PDA.
- Occluded SVG to the PDA (not shown).
As such, it is difficult to determine the exact location of the ischemia. There is also a second diagonal branch, which is diffusely diseased and supplied by epicardial collaterals.
I asked the referring MD to get a stress test. The patient had ischemia in the basal and mid anterior wall and anterolateral segments.
Our plan was to treat the high Ramus/OM1 and then proceed with the LAD CTO PCI. Here is the LCX PCI. We performed Culotte.
This is the dual injection angio for CTO PCI planning.
Here are some potential options for the CTO PCI.
Antegrade contrast modulation seemed to be our best bet. Here is the sequence for this rather novel crossing technique…
Proximal cap puncture with Gaia 2
The modified Carlino injection. Note the three breakout stains. In chronological order, these are a diagonal, a septal, and the distal true lumen.
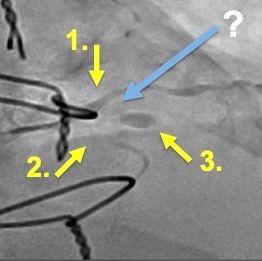
These are the three stains. Carlino has a name for this mechanism of CTO crossing. He calls it hydrodynamic contrast recanalization. Or HDR for short. This is a new term that you will be hearing about quite a bit in the future.
It can be difficult to tell if the ongoing stain is re-entry or infiltration into the extra plaque space. A retrograde injection clarifies this.
A Fielder XT without a tip bend is advanced across the channel made by the contrast under fluoroscopic guidance.
The micro catheter is an advanced over this wire. We confirm distal re-entry by means of pressure transduction and…
A distal tip injection.
Here is the final angiogram. This case highlights a new CTO crossing technique introduced by Mauro Carlino, and refined by us at UT. He calls it HDR as noted above. We have just submitted a paper describing the technique, and hopefully it will be accepted (soon!).
For our colleagues: CTO PCI is a mature field and several strategies for crossing CTOs have been developed. Most of them use wires. This ‘new’ technique is not so new – it is modification of an older technique which uses contrast injections. It is called Carlino after the interventionalist who described it.
