
LITERATURE REVIEW
Hema Manvi Koneru, MBBS,
Rajiv Gandhi Institute of Medical Sciences, Telangana, India
Divyasri Koneru, MBBS,
Dr.Pinnamaneni Siddartha Institute of Medical Sciences and Research Foundation, Andhra Pradesh, India.
Amanpreet Kaur, MBBS,
Government Medical College, Patiala, Punjab, India.
Amin H. Karim MD
Baylor College of Medicine, Houston, Texas
Introduction
Heart failure (HF) is a prevalent and serious condition associated with substantial morbidity and mortality. Management strategies have evolved, with recent focus on sodium-glucose cotransporter 2 (SGLT2) inhibitors potentially offering novel therapeutic benefits.
SGLT2 Inhibitors in HF with Reduced Ejection Fraction (HFrEF)
Studies have demonstrated that dapagliflozin, an SGLT2 inhibitor, significantly reduces the risk of worsening HF or cardiovascular death in patients with HFrEF. (1,3) The DAPA-HF trial, a pivotal phase 3 study, enrolled patients with New York Heart Association (NYHA) class II-IV symptoms and ejection fractions ≤ 40%. Results showed a reduction in the primary outcome (composite of worsening HF or cardiovascular death) among those treated with dapagliflozin compared to placebo (HR 0.74, 95% CI 0.65-0.85). This benefit was observed regardless of diabetes status, highlighting potential glucose-independent mechanisms of action.
SGLT2 Inhibitors in HF with Mildly Reduced or Preserved Ejection Fraction
Emerging evidence suggests that dapagliflozin may also benefit patients with HF and preserved or mildly reduced ejection fraction (HFpEF and HFmrEF). (2) The DELIVER trial randomized patients with HF and ejection fractions > 40% to dapagliflozin or placebo. Results indicated a reduction in the composite of worsening HF or cardiovascular death with dapagliflozin (HR 0.82, 95% CI 0.73-0.92). Moreover, improvements in symptom burden were noted, supporting potential broad utility across HF phenotypes.
Mechanisms of Action
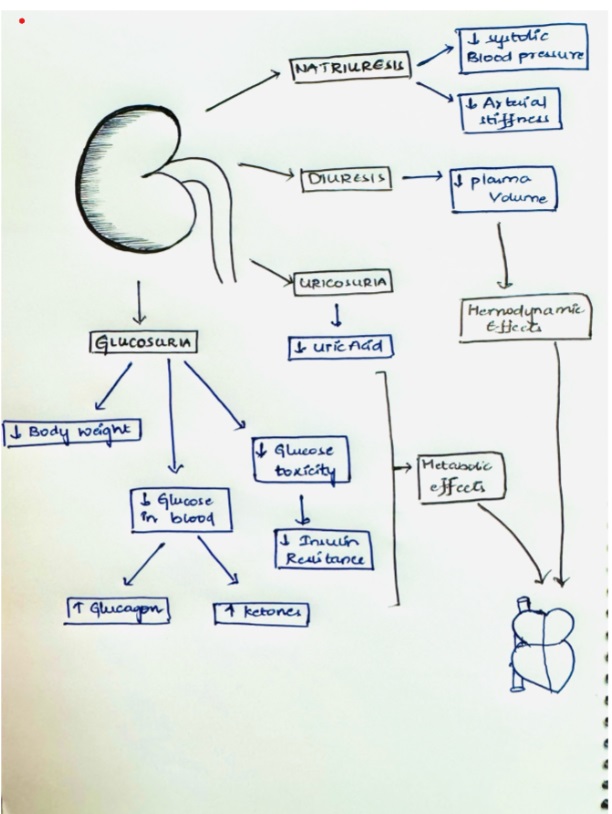
Beyond glycemic control, SGLT2 inhibitors like dapagliflozin may exert beneficial effects in HF through mechanisms including improved cardiac remodeling, reduced sodium retention, decrease plasma volume, and potential metabolic modulation. These mechanisms contribute to improved hemodynamics and reduced cardiovascular morbidity and mortality, as observed in clinical trials.
Contraindication
- eGFR < 30mL/minute/1.73 m2
Safety and Tolerability
Safety profiles across trials indicate that dapagliflozin is generally well tolerated in HF patients, with adverse event rates comparable to placebo. Common side effects include volume depletion and renal dysfunction (Acute kidney injury due to dehydration), which are manageable with appropriate monitoring. Other severe side effects are euglycemic diabetic ketoacidosis, allergic reaction and genital infections (mostly fungal).
- Canagliflozin increase the risk of lower limb amputation and bone fractures.
Clinical Implications and Future Directions
The efficacy of SGLT2 inhibitors in reducing HF-related events underscores their potential as adjunctive therapy in standard HF management. Future research should focus on optimizing patient selection, exploring combination therapies, and elucidating long-term benefits and risks in diverse patient populations.
Conclusion
SGLT2 inhibitors like dapagliflozin show great promise in improving outcomes for patients with heart failure. These medications not only reduce cardiovascular risks but also improve quality of life, highlighting their potential as essential elements of comprehensive heart failure treatment strategies.
References
- McMurray JJV, Solomon SD, Inzucchi SE, Køber L, Kosiborod MN, Martinez FA, Ponikowski P, Sabatine MS, Anand IS, Bělohlávek J, Böhm M, Chiang CE, Chopra VK, de Boer RA, Desai AS, Diez M, Drozdz J, Dukát A, Ge J, Howlett JG, Katova T, Kitakaze M, Ljungman CEA, Merkely B, Nicolau JC, O’Meara E, Petrie MC, Vinh PN, Schou M, Tereshchenko S, Verma S, Held C, DeMets DL, Docherty KF, Jhund PS, Bengtsson O, Sjöstrand M, Langkilde AM; DAPA-HF Trial Committees and Investigators. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N Engl J Med. 2019 Nov 21;381(21):1995-2008. doi: 10.1056/NEJMoa1911303. Epub 2019 Sep 19. PMID: 31535829.
- Solomon SD, McMurray JJV, Claggett B, de Boer RA, DeMets D, Hernandez AF, Inzucchi SE, Kosiborod MN, Lam CSP, Martinez F, Shah SJ, Desai AS, Jhund PS, Belohlavek J, Chiang CE, Borleffs CJW, Comin-Colet J, Dobreanu D, Drozdz J, Fang JC, Alcocer-Gamba MA, Al Habeeb W, Han Y, Cabrera Honorio JW, Janssens SP, Katova T, Kitakaze M, Merkely B, O’Meara E, Saraiva JFK, Tereshchenko SN, Thierer J, Vaduganathan M, Vardeny O, Verma S, Pham VN, Wilderäng U, Zaozerska N, Bachus E, Lindholm D, Petersson M, Langkilde AM; DELIVER Trial Committees and Investigators. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N Engl J Med. 2022 Sep 22;387(12):1089-1098. doi: 10.1056/NEJMoa2206286. Epub 2022 Aug 27. PMID: 36027570.
- Nassif ME, Windsor SL, Borlaug BA, Kitzman DW, Shah SJ, Tang F, Khariton Y, Malik AO, Khumri T, Umpierrez G, Lamba S, Sharma K, Khan SS, Chandra L, Gordon RA, Ryan JJ, Chaudhry SP, Joseph SM, Chow CH, Kanwar MK, Pursley M, Siraj ES, Lewis GD, Clemson BS, Fong M, Kosiborod MN. The SGLT2 inhibitor dapagliflozin in heart failure with preserved ejection fraction: a multicenter randomized trial. Nat Med. 2021 Nov;27(11):1954-1960. doi: 10.1038/s41591-021-01536-x. Epub 2021 Oct 28. PMID: 34711976; PMCID: PMC8604725.
- Petrie MC, Verma S, Docherty KF, Inzucchi SE, Anand I, Belohlávek J, Böhm M, Chiang CE, Chopra VK, de Boer RA, Desai AS, Diez M, Drozdz J, Dukát A, Ge J, Howlett J, Katova T, Kitakaze M, Ljungman CEA, Merkely B, Nicolau JC, O’Meara E, Vinh PN, Schou M, Tereshchenko S, Køber L, Kosiborod MN, Langkilde AM, Martinez FA, Ponikowski P, Sabatine MS, Sjöstrand M, Solomon SD, Johanson P, Greasley PJ, Boulton D, Bengtsson O, Jhund PS, McMurray JJV. Effect of Dapagliflozin on Worsening Heart Failure and Cardiovascular Death in Patients With Heart Failure With and Without Diabetes. JAMA. 2020 Apr 14;323(14):1353-1368. doi: 10.1001/jama.2020.1906. Erratum in: JAMA. 2021 Apr 6;325(13):1335. doi: 10.1001/jama.2021.2802. PMID: 32219386; PMCID: PMC7157181.
- Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, Silverman MG, Zelniker TA, Kuder JF, Murphy SA, Bhatt DL, Leiter LA, McGuire DK, Wilding JPH, Ruff CT, Gause-Nilsson IAM, Fredriksson M, Johansson PA, Langkilde AM, Sabatine MS; DECLARE–TIMI 58 Investigators. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med. 2019 Jan 24;380(4):347-357. doi: 10.1056/NEJMoa1812389. Epub 2018 Nov 10. PMID: 30415602.
