Heart Failure with Preserved Ejection Fraction and Atrial Fibrillation: What was first, the Egg or the Chicken?
Laiba Ejaz Karachi Institute of Medical Sciences.
Samuel Sotelo Hernandez Autonomous University of Durango-Cappus Zacatecas
Amin H. Karim MD Methodist Academy of Medicine, Houston, Texas
Abstract A 68-year-old African American man presented with recurrent lower extremity edema without dyspnea or chest pain. His history included hypertension, hyperlipidemia, and obesity. Evaluation revealed atrial fibrillation with a controlled ventricular rate and echocardiographic findings consistent with heart failure with preserved ejection fraction (HFpEF). Secondary causes such as deep venous thrombosis were excluded. The patient was managed with metoprolol and diuretics for rate and volume control, losartan and hydrochlorothiazide for hypertension, apixaban for anticoagulation, and amiodarone for rhythm stabilisation. After a year of persistent atrial fibrillation, elective cardioversion successfully restored sinus rhythm following confirmation of the absence of atrial thrombus on transesophageal echocardiography. The patient remained clinically stable on subsequent follow-up visits.
Introduction Atrial fibrillation (AF) and heart failure with preserved ejection fraction (HFpEF) are common cardiovascular conditions that frequently coexist, particularly in older, hypertensive, and obese patients. AF can exacerbate HFpEF by impairing atrial contribution to ventricular filling, while HFpEF may predispose to atrial remodelling and subsequent arrhythmia, creating a complex bidirectional relationship. Both conditions independently increase morbidity and mortality and pose challenges in diagnosis and management, especially when symptoms such as edema or fatigue are subtle or overlapping. Understanding the temporal relationship between AF and HFpEF is critical for optimizing therapy, including rate versus rhythm control, anticoagulation, and management of comorbidities. This case highlights a patient with recurrent lower extremity edema, AF, and HFpEF, raising the clinical question of which condition preceded the other and illustrating the importance of individualized, comprehensive cardiovascular care.
Case Presentation A 68-year-old African American man presented to the clinic with complaints of recurrent fluid buildup, mainly in his lower extremities, as noted by his primary care physician. He denied dyspnea, chest pain, orthopnea, or paroxysmal nocturnal dyspnea. His medical history included hypertension, hyperlipidemia, and obesity. He reported occasional alcohol use and denied smoking. His family history was significant for coronary artery disease, hypertension, hyperlipidemia, and diabetes mellitus. On examination, his weight was 280 lbs (127 kg) and height 73 inches, yielding a BMI of 37.7 kg/m2, consistent with Class I obesity. Blood pressure ranged between 135–145/75–85 mmHg, and his pulse was irregular at 58–70 beats per minute.
Laboratory investigations revealed a normal HbA1c and a lipid profile with total cholesterol 222 mg/dL, HDL 67 mg/dL, LDL 149 mg/dL, and triglycerides 60 mg/dL. An electrocardiogram (EKG) (figure 1) obtained during the initial visit showed atrial fibrillation with a controlled ventricular rate of approximately 58 beats per minute. A subsequent 2D echocardiogram demonstrated a preserved left ventricular ejection fraction of 60–65% and mild left atrial enlargement—findings consistent with heart failure with preserved ejection fraction (HFpEF). Chest X-ray showed chronic airway changes and mild atherosclerosis, while Doppler ultrasound ruled out deep venous thrombosis. The patient was started on metoprolol and diuretics for rate and volume control, along with losartan and hydrochlorothiazide for blood pressure management. Anticoagulation with Eliquis (apixaban) and rhythm control with amiodarone was initiated and continued for over a year without spontaneous conversion to sinus rhythm (figure 2). He subsequently underwent elective cardioversion, which successfully restored sinus rhythm (figure 3) A transesophageal echocardiogram prior to the procedure confirmed the absence of thrombus in the left atrium or left atrial appendage. The patient continued regular follow-up and remained clinically stable thereafter.
Discussion This case highlights the complex interplay between atrial fibrillation (AF), hypertension, obesity, and heart failure with preserved ejection fraction (HFpEF) in an older African American male. The patient’s presentation with peripheral edema, in the absence of dyspnea or orthopnea, emphasises that HFpEF can manifest subtly and that careful evaluation of cardiovascular risk factors and cardiac rhythm is essential for accurate diagnosis and management (1,2). Atrial fibrillation is a common arrhythmia in elderly individuals, often associated with structural heart changes such as left atrial enlargement and diastolic dysfunction. In this patient, chronic hypertension and obesity likely contributed to increased left ventricular stiffness and impaired relaxation, leading to diastolic dysfunction and, consequently, HFpEF (3,4). The echocardiographic findings of preserved left ventricular ejection fraction (60–65%) with mild left atrial enlargement are consistent with this diagnosis. The irregularly irregular rhythm on electrocardiogram confirmed the presence of AF, while the controlled ventricular rate suggested adequate rate control with beta-blocker therapy (5). HFpEF accounts for nearly half of all heart failure cases, and its prevalence continues to rise in parallel with obesity, hypertension, and metabolic syndrome (1,6). Pathophysiologically , the combination of increased ventricular wall stress, endothelial dysfunction, and myocardial fibrosis results in elevated filling pressures despite normal systolic function (7). This leads to symptoms such as lower extremity edema, exercise intolerance, or mild dyspnea, which may fluctuate depending on volume status. Importantly, obesity is a key modifiable factor that exacerbates both HFpEF and AF by promoting systemic inflammation, left atrial remodelling, and neurohormonal activation (6,7). The management of this patient was appropriately focused on controlling heart rate, optimizing blood pressure, managing volume status, and preventing thromboembolic events. Beta-blocker therapy (metoprolol) was effective for rate control, while diuretics addressed the peripheral edema. Losartan and hydrochlorothiazide provided additional blood pressure control and diuresis. Given the patient’s CHA2DS2-VASc score—elevated due to age, hypertension, and heart failure—anticoagulation with apixaban was warranted to reduce the risk of stroke, which is fivefold higher in individuals with AF (5,8). Despite more than a year of rate control and anticoagulation, the patient did not experience spontaneous reversion to sinus rhythm. Therefore, elective cardioversion was pursued, preceded by transesophageal echocardiography to rule out intracardiac thrombus. The successful restoration of sinus rhythm improved cardiac efficiency and potentially reduced the risk of HF progression (9). Ongoing rhythm surveillance is essential, as recurrence of AF is common, particularly in patients with underlying structural heart disease and obesity (10). From a preventive perspective, aggressive risk factor modification remains a cornerstone of long -term management. Weight reduction, dietary sodium restriction, and increased physical activity can improve diastolic function and reduce AF recurrence (1,2). Additionally, lipid lowering with statin therapy is indicated given the elevated LDL cholesterol level (149 mg/dL), further reducing cardiovascular risk (3,6).
In summary, this case underscores the importance of a multidisciplinary approach in managing AF and HFpEF , particularly in patients with multiple cardiovascular risk factors. Optimal control of hypertension, obesity, and dyslipidemia, combined with rhythm management and anticoagulation, can lead to favorable clinical outcomes. The patient’s successful cardioversion and stable follow-up course demonstrate that with comprehensive care, symptom control and maintenance of sinus rhythm are achievable in this complex patient population.
References:
Kittleson MM, Panjrath GS, Amancherla K, et al. 2023 ACC Expert Consensus Decision Pathway on Management of Heart Failure With Preserved Ejection Fraction. J Am Coll Cardiol. 2023;81(18):1835–78. doi:10.1016/j.jacc.2023.03.393
American College of Cardiology. 2024 ACC Expert Consensus Decision Pathway on Clinical Assessment, Management, and Trajectory of Patients Hospitalized With Heart Failure. J Am Coll Cardiol. 2024. doi:10.1016/j.jacc.2024.06.002
American College of Cardiology/American Heart Association. 2024 Update to the 2020 ACC/AHA Clinical Performance and Quality Measures for Adults With Heart Failure. Circ Heart Fail/HCQ.
doi:10.1161/HCQ.0000000000000132
Riccardi M, et al. Current Treatment of Heart Failure with Preserved Ejection Fraction. J Clin Med. 2025;14(15):5406. doi:10.3390/jcm14155406
Romanò M, et al. Heart Failure Syndromes: Different Definitions of Ejection Fraction and Implications. J Clin Med. 2025;14(14):5090. doi:10.3390/jcm14145090
Spotlight on the 2024 ESC/EACTS Management of Atrial Fibrillation. Eur Heart J Cardiovasc Pharmacother. 2025. doi:10.1093/ehjcvp/pvad014
In 1977 I wrote up a small booklet called CLINICAL STUDENTS COMPANION and had it published by AzamSons, a book seller across from Dow Medical College. It was basically notes on General Medicine I made for the Final Professional MBBS Exam. It was common for oral examiners to ask for causes of symptoms, signs or abnormal lab values. This helped junior students to brush up on lists of causes which one could not find easily from text books of Medicine like Davidson or Harrison or Cecil Loeb. I then published two more editions wht last one being what is being uploaded here, a 260 page book with illustrations. The third edition was typed by me on the old manual Smith Corona portable type-writer.
One technique we learnt from teachers like Prof. S.M Rab (with whom I did my first intership in Medicine at Jinnah PostGraduate Medical Center, Karachi) was to think about the causes of a presentation or symptom or sign one at a time. If patient has 2-4 signs think of all the causes separately and try to figure what runs common to all the lists. This may lead one to correct diagnosis. For example when presented with Fever of Unknown Origin, think of the causes and if the patient also has anemia and splinter hemorrhages, one would find that bacterial endocarditis is present in all the 3 lists. Same for other problems.
Hope you enjoy reading. Mind you this is 45 years ago and applies to diseases found commonly in Pakistan and India. It’s value at this stage may be more historical than actual since everything now is a mouse click away on ChatGPT! 🙂 Amin H. Karim MD September 25 2025
A CASE OF POSTOPERATIVE COMPLICATION OF SURGICAL MITRAL VALVE REPLACEMENT.
Amin H. Karim MD
CASE: A 71 year olf Caucasian male with history of hypertension and hyperlipidemia, and chronic atrial fibrillation, developed non-rheumatic mitral valve regurgitation secondary to mitral valve prolapse, which had gradually progressed over a decade years to severe regurgitation, accompanied by moderately severe tricuspid regurgitation. Patient tolerated the valvular lesions for many years till he became symptomatic with NYHA Class III dyspnea and agreed for intervention.
CARDIAC MRI: In November 2024, cardiac MRI revealed bi-leaflet mitral valve prolapse, with severe left atrial enlargement and moderate tricuspid regurgitation. The global ejection fraction was 65% with biventricular dilatation, and basal and mid inferolateral wall scarring. Mitral and tricuspid annulus were dilated.
TWO DIMENSIONAL ECHOCARDIOGRAM: On Echocardiogram, right ventricular function was low normal. Left ventricular ejection fraction was normal. There was mitral valve prolapse due to myxomatous degeneration, severe mitral regurgitation with regurgitation fraction of 51% and estimated regurgitant volume of 56 ml. Pulmonary artery pressures were normal. Cardiac catheterization showed normal coronaries
With a low BMI and good overall health, he was felt by the cardiovascular surgeon to be low risk for surgery and MitraClip therefore not warranted.
MITRAL VALVE REPAIR SURGERY: Mitral valve repair with a 34 mm physio 2 flexible annuloplasty ring; Intra-aortic balloon pump; Tricuspid valve repair with a 28 mm triad rigid ring; Biatrial maze utilizing the encompass clamp, RF clamp and cryoprobe; Left atrial appendage ligation with a 45 mm atrial cure mini atrial clip:
Following mitral valve repair there was no mitral regurgitation with a long segment of coaptation beneath the annular plane. The transmitral gradient was 1 mm Hg. Similarly following tricuspid valve repair there was no regurgitation with the trans tricuspid valve gradient of 1 mm. Following bi-atrial maze procedure, the patient converted to sinus rhythm. However, when the cardio pulmonary bypass was reversed and the patient was being closed, he went to ventricular fibrillation followed by defibrillation. Frequent PVCs were observed. Intravenous amiodarone and magnesium were started; His blood pressure started to drop and vasopressors were increased and intra-aortic balloon placed. His hemodynamics improved and was watched in the OR with echo. There was inferior wall hypokinesis. He was maintained on low dose dobutamine, vasopressin and norepinephrine. His global ejection fraction was reasonable; chest was closed, but before he could be transferred out of OR he developed ventricular fibrillation again. His chest was opened and direct cardiac massage and cardioversion done with return of circulation. ECMO (Extracorporeal Membrane Oxygenation) was initiated. He was transferred to the cardiac cath lab and underwent emergency coronary angiography.
CORONARY INTERVENTION: Coronary angiography showed the dominant left circumflex was occluded in the mid potion.
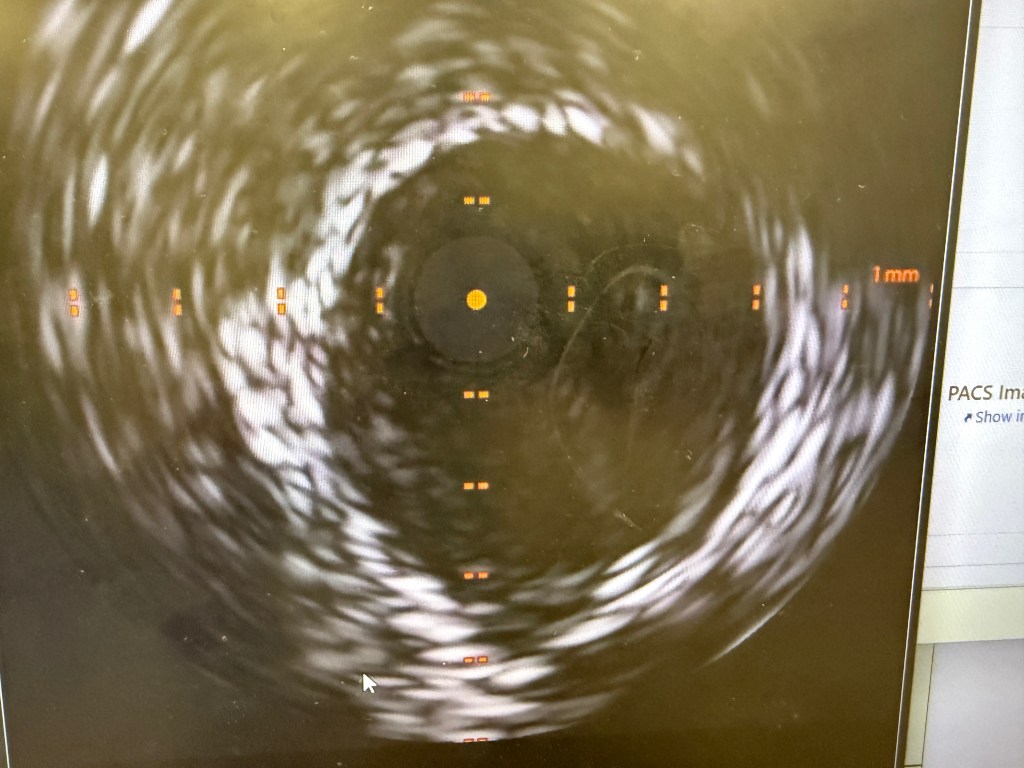
IVUS showed possible edema around the left circumflex and it was felt that the circumflex was occluded due to pressure from the mitral valve ring. Stent was placed with recanalization. Impella was placed in the cath lab and the intra-aortic balloon was removed.
Intavascular Ultrasound (IVUS) shows the edema/hematoma? aeound the left vircumflex artery.
A 3.5 mm x 32 mm Synergy drug eluting stent was placed in the mid circumflex coronary artery with a good result. The intra-aortic balloon was removed.
INTENSIVE CARE UNIT: Patient remained with supported blood pressure, with severe anemia needing multiple blood transfusions. Transesophageal echo showed severely depressed right and left ventricular systolic function. Patient was taken back to O.R. for exploration and washout. On return to ICU noted to have ST elevation in lead VII. Taken back to cath lab and coronary angiography done showing that the circumflex stent was patent.
FOLLOWUP: 10 days after mitral and tricuspid valve repair and coronary intervention, patient is off ECMO, and on Impella support. He is awake but does not follow commands. His global ejection fraction on echocardiogram is mildly depressed (40-45%) with trace of mitral and tricuspid regurgitation.
By Ana María Sierra Valiente Universidad Anáhuac México Norte Amin H. Karim MD, Clinical Associate Professor Baylor College of Medicine, Houston, Texas.
Interrupting Anticoagulants for Surgery: Guidelines, Risk Stratification, and Clinical Decision-Making.
Raya Kharboutli PA-S2 University of Texas Medical Branch
Regina Medina Urrutia Universidad Anahuac Campus Xalapa
Anticoagulants are a class of medications used to prevent and treat thromboembolic events such as stroke, deep vein thrombosis, and pulmonary embolism. These agents are divided into two main categories: antiplatelet agents and anticoagulants that inhibit coagulation factors. Understanding their mechanisms of action is critical for making safe perioperative decisions.
Antiplatelet agents like aspirin irreversibly inhibit cyclooxygenase (COX-1), preventing the production of thromboxane A₂, a molecule essential for platelet activation. As a result, platelet aggregation is impaired for the lifespan of the platelet, which is approximately 7-9 days (1). Clopidogrel, a P2Y12 receptor inhibitor, irreversibly blocks ADP receptors on the platelet surface, further preventing platelet activation and aggregation. Following discontinuation, platelet function typically returns to baseline within about 5 days (2). Warfarin is a vitamin K antagonist that works by inhibiting vitamin K epoxide reductase, an enzyme required for the activation of clotting factors II, VII, IX, and X. Warfarin has a delayed onset of action, with therapeutic anticoagulation typically achieved within 2 to 3 days. Monitoring is performed using International Normalized Ratio (INR), and full reversal of anticoagulant effect takes approximately 3 to 5 days. This process can be expedited with the administration of vitamin K (3). Direct oral anticoagulants (DOACs) are a newer class of medications with more predictable pharmacokinetics. These include factor Xa inhibitors such as apixaban, rivaroxaban, and edoxaban, which inhibit factor Xa, thereby blocking the conversion of prothrombin to thrombin. Additionally, dabigatran is a direct thrombin inhibitor (Factor IIa), which prevents the conversion of fibrinogen to fibrin, the final step in clot formation (4).
The type of anticoagulant used plays an important role in how far in advance it should be discontinued:
Warfarin should usually be stopped 5 days before surgery to allow the INR to return to a safe range (usually <1.5) (11).
Direct oral anticoagulants (DOACs) like apixaban, rivaroxaban, dabigatran, and edoxaban are usually suspended 24–72 hours before surgery, depending on the bleeding risk of the procedure and the patient’s kidney function. For example, dabigatran is mostly eliminated by the kidneys, so patients with renal impairment need to stop it even earlier (11).
This classification and understanding of mechanisms provide a foundation for evaluating how and when these agents should be temporarily discontinued prior to surgical or invasive procedures, based on the individual agent, patient thrombotic risk, and the bleeding risk associated with the procedure
Interrupting anticoagulation before a procedure is often necessary to reduce the risk of excessive bleeding during or after surgery. Anticoagulants and antiplatelet agents impair the body’s ability to form clots, which is beneficial for preventing thrombosis but can lead to significant complications when tissue trauma or vascular injury is expected. The decision to pause these medications is a balance between two major risks: bleeding and thrombosis. For procedures with a high bleeding risk, such as major surgeries, spinal or epidural anesthesia, and certain endoscopic or urologic procedures, continued anticoagulation can increase the chance of uncontrolled bleeding, hematoma formation, or the need for transfusions (5). On the other hand, abruptly stopping antithrombotic therapy, especially in high-risk patients (such as those with recent stroke, atrial fibrillation, or coronary stents), may raise the risk of life-threatening thromboembolic events (7). Therefore, clinicians must evaluate the type of anticoagulant, the patient’s thrombotic risk, and the bleeding risk of the procedure to determine the safest perioperative plan. In many cases, temporary interruption with or without bridging therapy allows for safe procedural outcomes while minimizing harm from both bleeding and clot formation (6).
In cardiology, several invasive procedures carry moderate to high bleeding risk and typically require temporary interruption of anticoagulant or antiplatelet therapy. The decision depends on the type of medication, the procedure’s bleeding risk, and the patient’s thromboembolic risk. For cardiac surgery, such as coronary artery bypass grafting (CABG) or valve replacement, both antiplatelet agents and anticoagulants are usually interrupted. Aspirin is often continued unless bleeding risk is very high but clopidogrel is typically discontinued at least 5-7 days before surgery to minimize perioperative bleeding (8). Warfarin is usually stopped 5 days prior, aiming for an INR of less than 1.5 on the day of the surgery. In patients at high thromboembolic risk such as mechanical valve or atrial fibrillation with prior stroke, bridging with low molecular weight heparin (LMWH) may be considered. Direct oral anticoagulants are typically held for 2-3 days before major cardiac surgery, with the exact timing depending on renal function.
For pacemaker or implantable cardioverter-defibrillator (ICD) insertion, the bleeding risk is considered moderate. Aspirin may be continued in most cases, but clopidogrel should be stopped 5-7 days prior, especially if dual antiplatelet therapy is not mandatory at the time. DOACs are commonly interrupted 24-48 hours before the procedure, depending on renal function and Warfarin is often continued at a therapeutic INR for minor device procedures, but only interrupted in high-bleeding-risk cases (9). Percutaneous coronary intervention (PCI) presents a unique challenge, especially in patients already on dual antiplatelet therapy (DAPT). These procedures are rarely elective if DAPT is indicated. If non-urgent PCI must be delayed, clopidogrel is held 5-7 days and DOACs for 48-72 hours prior (10).
Ultimately, the goal is to minimize both bleeding and thrombotic complications by tailoring medication interruption based on the procedure type, medication half-life, and patient risk factors.
The management of patients going under anesthesia for surgery is a really common challenge due to the decision to suspend or not the anticoagulants the patients are on. Many protocols can be followed to help make the decision. One of these protocols is to evaluate both the risk of bleeding and thromboembolism, and it’s important to know the dosage of the anticoagulant and the reasons why the patient is taking the specific anticoagulant.
First of all, the risk of bleeding needs to be estimated. One way is the HAS-BLEED score, which will assess the following risk factors such as hypertension, abnormal liver or renal functions, stroke, bleeding, labile INRs, elderly patients (>65 years), and the use of drugs or alcohol. The second step is to estimate the thromboembolic risk, and to do that, age and comorbidities need to be evaluated (12). If the patient has had a recent event of DVT or PE, the decision is based on the diagnosis, but in this scenario, the surgery is delayed as much as possible. Once the two important risks are evaluated, the duration to interrupt the anticoagulant is going to depend on which medication the patient is on. If the patient has low kidney or liver function, we might need additional consideration. In general, almost every procedure, the anticoagulant must be suspended if the risk of bleeding or high thrombotic risk, but if the risk is low isn’t necessarily necessary to stop the medication (12).
There are really selected procedures where we can keep using the anticoagulant, like in a dental extraction, skin biopsy, or a cataract surgery, but also in a procedure like a cardiac implant electronic device, it’s not necessary to stop taking them. The ERHA states that if the patient is going to be under the implantation of a cardiac electronic device like a pacemaker, the patient should continue the anticoagulant perioperatively (13). Unless the patient has a risk of a thromboembolic event and is under warfarin or DOCAs, the medication should be suspended temporarily. In the case of any endovascular procedures like an angioplasty, a meta-analysis randomly shows that patients who were under warfarin and didn’t interrupt while undergoing the procedure were associated with lower risks of complications compared with those who interrupted the warfarin perioperatively (11).
In patients with high thrombotic risk, it may be necessary to use bridging therapy with low-molecular-weight heparin (LMWH) during the time the oral anticoagulant is stopped. However, the BRIDGE trial showed that bridging in patients with non-valvular atrial fibrillation and moderate thrombotic risk increased the risk of bleeding without significantly reducing thromboembolic events (14). Therefore, bridging should only be considered in selected high-risk patients.
When using spinal or epidural anesthesia, anticoagulants increase the risk of spinal hematoma, which can cause permanent paralysis. According to the American Society of Regional Anesthesia (ASRA), anticoagulants such as DOACs should be stopped at least 72 hours before any neuraxial procedures, and specific guidelines should be followed for restarting the medication (15).
Individual characteristics such as renal or liver function, age, history of bleeding, and the use of other medications like antiplatelet agents or NSAIDs, must also be considered when deciding whether to stop anticoagulants before surgery (11).Restarting anticoagulants too soon can lead to postoperative bleeding, while delaying them too long can cause thromboembolism. In general, anticoagulants can be restarted 24–48 hours after surgery if bleeding is under control and the patient is stable (11).
References:
Haut, E. R., Pronovost, P. J., & Owings, J. T. (2016). Thromboembolic complications in trauma patients. Trauma Surgery & Acute Care Open, 1(1), e000022. https://doi.org/10.1136/tsaco-2015-000022
Pannucci, C. J., & Dresher, M. (2017). Postoperative venous thromboembolism: Risk factors and prevention. International Journal of Environmental Research and Public Health, 14(3), 301. https://doi.org/10.3390/ijerph14030301
Hirsh, J., Guyatt, G., Albers, G. W., Harrington, R., & Schünemann, H. J. (2008). Antithrombotic and thrombolytic therapy: American College of Chest Physicians evidence-based clinical practice guidelines (8th edition). Circulation, 107, 1692–1700. https://doi.org/10.1161/01.CIR.0000063575.17904.4E
Guyatt, G. H., Akl, E. A., Hirsh, J., Crowther, M., Gutterman, D. D., & Schünemann, H. J. (2022). American College of Chest Physicians Antithrombotic Guidelines. Chest, 161(5), 1272–1302. https://doi.org/10.1016/j.chest.2022.01.032
Nasser, M., Jaffer, A. K., Milani, R. V., & Lavie, C. J. (2021). Perioperative management of anticoagulants in patients undergoing elective procedures. Perioperative Medicine, 10(1), 1–9. https://doi.org/10.1186/s13741-020-00170-4
Kakar, T. S., Elbaroni, M., & Kang, N. (2020). Bridging anticoagulation therapy in patients undergoing procedures: A literature review. Cardiology Research, 11(5), 328–334. https://doi.org/10.14740/cr1110
Douketis, J. D., Spyropoulos, A. C., Duncan, J., Carrier, M., Le Gal, G., & Tafur, A. J. (2021). Perioperative management of anticoagulant and antiplatelet therapy. Thrombosis Journal, 19(1), 29. https://doi.org/10.1186/s12959-021-00279-6
Douketis, J. D., Spyropoulos, A. C., Kaatz, S., Becker, R. C., Caprini, J. A., Dunn, A. S., … & Schulman, S. (2015). Perioperative bridging anticoagulation in patients with atrial fibrillation. New England Journal of Medicine, 373(9), 823–833. https://doi.org/10.1056/NEJMoa1302946
Kaicker, J., Mokrzycki, M. H., & Salvador, D. (2024). Bleeding risk assessment and anticoagulant management during surgery. PubMed. https://pubmed.ncbi.nlm.nih.gov/38320132/
Heidbuchel, H., Verhamme, P., Alings, M., Antz, M., Hacke, W., Oldgren, J., … & Lip, G. Y. H. (2015). Updated European Heart Rhythm Association practical guide on the use of non-vitamin K antagonist anticoagulants in patients with non-valvular atrial fibrillation. Europace, 17(10), 1467–1507. https://doi.org/10.1093/europace/euv309
Macedo, A. F., Bell, J., McCarron, C., & Fahey, T. (2018). Interventions to improve appropriate prescribing of anticoagulants in atrial fibrillation: A systematic review. BMC Cardiovascular Disorders, 18(1), 24. https://doi.org/10.1186/s12872-018-0762-1
Sarai Anayansi Zárate Chávez Universidad Anáhuac campus Oaxaca
Juan Pablo García Guzmán Universidad Anáhuac Mexico campus Norte
Amin H. Karim MD Institute of Academic Medicine, Houston, Texas Weill Medical College of Cornell University.
What Is a Blood Clot? A blood clot also referred to as a thrombus (plural: thrombi), intravascular clot, or coagulum is a gelatinous or semi-solid mass of coagulated blood that forms within the circulatory system. When such a clot develops in the deep venous system, most commonly in the lower limbs, it is termed deep vein thrombosis (DVT), although it can also occur in the upper extremities. A major complication of DVT is embolization, in which one or more thrombi detach and travel through the venous circulation often originating in the legs, pelvis, or groin and reach the pulmonary arteries, leading to a pulmonary embolism (PE). This condition can be life-threatening and requires immediate medical intervention. Thrombus Formation and Intracardiac Clot Dynamics A thrombus also referred to as a clot, blood clot, embolus (when mobile), or thromboembolus (when causing obstruction) is the result of a complex interaction between endothelial injury, abnormal blood flow (stasis or turbulence), and a hypercoagulable state, often summarized by Virchow’s triad. In the setting of acute vascular injury, particularly in acute coronary syndrome (ACS), clot formation begins with platelet adhesion to exposed subendothelial proteins at sites of plaque rupture or erosion. Once adhered, platelets become activated, change shape, and release a variety of pro-thrombotic substances including thromboxane A2, ADP, and serotonin, promoting further platelet activation and local vasoconstriction. The surface expression of glycoprotein IIb/IIIa receptors increases, facilitating platelet aggregation through fibrinogen bridging. Concurrently, the coagulation cascade is triggered, leading to thrombin generation. Thrombin amplifies platelet activation and converts fibrinogen into fibrin, which stabilizes the growing thrombus. As fibrin is laid down, a stable platelet-fibrin thrombus forms, which may partially or completely obstruct the vessel. If embolized, fragments of the thrombus may lodge downstream, causing ischemia or infarction. Intracardiac thrombi form under somewhat different circumstances, often related to blood stasis or structural heart disease. In the left ventricle, thrombi can arise after anterior myocardial infarction, especially with regional wall motion abnormalities such as apical akinesis or dyskinesis. In non-ischemic dilated cardiomyopathy, the risk is lower but still present, particularly when left ventricular ejection fraction is severely reduced. The left atrium, particularly the left atrial appendage, is a common site for thrombus formation in patients with atrial fibrillation, atrial flutter, or significant mitral valve disease. Even in sinus rhythm, atrial mechanical dysfunction—as in cardiac amyloidosis—can predispose to thrombus formation. On the right side of the heart, thrombi may form in cases of central venous catheters, intracardiac devices, severe right ventricular dysfunction, or hypercoagulable states. Additionally, mechanical prosthetic valves, especially with inadequate anticoagulation, are a high-risk source of thrombus formation and systemic embolism. Paradoxical embolism can occur in the presence of a patent foramen ovale (PFO) or atrial septal defect (ASD), where venous thrombi bypass the pulmonary circulation and enter the systemic arterial system through a right-to-left intracardiac shunt.
Diagnosis: Tests The main diagnostic tests for detecting thrombi in the left ventricle are transthoracic echocardiography (TTE) and cardiac magnetic resonance imaging (CMRI) with delayed gadolinium enhancement. TTE is the most used initial technique due to its availability and low cost: however, its sensitivity is limited (approximately 21-35%), although its specificity is high (95-98%). The use of intravenous contrast agents in TTE improves sensitivity (up to 64%) without losing specificity. Transthoracic echocardiography has been utilized for identifying left ventricular thrombi since the early 1980s. In recent years, the introduction of echocardiographic contrast agents has improved detections accuracy, particularly in patients with suboptimal acoustic windows. TTE remains the initial diagnostic modality of choice for evaluating left ventricular thrombus. However, its limitations such as difficulty imaging patients with poor acoustic windows, can lead to considerable interobserver variability, potentially compromising diagnostic reliability. Cardiac magnetic resonance offers a diagnostic edge over echocardiography by allowing both myocardial tissue characterization and dynamic imaging. With recent advancements in imaging sequences and the use of paramagnetic contrast agents to enhance blood pool visualization, late gadolinium enhancement CMR may offer superior sensitivity for detecting left ventricular thrombi. Recent epidemiologic tests have provided that the incidence of left ventricular thrombus, using optimal imaging modalities, can reach up to 15% in patients with ST segment elevation myocardial infarction and up to 25% in those with anterior myocardial infarction. Although a standard transthoracic echocardiogram is frequently used for initial screening, its low sensitivity in detecting left ventricular thrombus requires the use of contrast (when not contraindicated) and/or cardiac MRI when there is a high pretest probability. Transesophageal echocardiography does not provide advantages for visualizing the ventricular apex and is not recommended as a second-line method for ventricular thrombi. The first study that was able to compare the diagnostic accuracies of CMRI, contrast TTE and noncontrast TTE was performed by Weinsaft et al. That demonstrated that even with administration of echocardiographic contrast agents, CMRI was still considerably more accurate modality in terms of thrombus detection. CMR with late gadolinium enhancement is the gold standard, with a sensitivity of 82-88% and specificity of 99-100%, as it allows differentiation of the thrombus (avascular without enhancement) from the surrounding myocardium. It is especially recommended when TTE (even with contrast) is not diagnostic or clinical suspicion persists. Cardiac computed tomography can incidentally detect thrombi, but it is not validated for this purpose Precise detection of left ventricular thrombi is crucial, as it frequently guides the initiation of anticoagulation therapy to reduce the risk of embolic complications. While current guidelines suggest that starting anticoagulation may be reasonable in patients with strong suspicion of thrombus such as those with apical akinesis or dyskinesis even without visible thrombus, selecting the most appropriate imaging modality is essential to ensure timely and evidence-based therapeutic decisions.
Complications The main complications of thrombi in the left ventricle are systemic embolic events, especially ischemic stroke and peripheral arterial embolisms. Embolization occurs because the thrombus can detach and migrate into systemic circulation, affecting organs such as the brain, kidneys, spleen, or extremities. The risk of embolization is particularly high in the first few weeks after an acute myocardial infarction and can reach up to 22% depending on the morphology and follow up of the thrombus. The incidence of systemic embolic events in patients with left ventricular thrombi varies depending on the population and clinical context. In patients with acute myocardial infarction (AMI), the incidence of left ventricular thrombus is 3.5% to 7.1% after previous AMI when cardiac magnetic resonance imaging is used, and the incidence of systemic embolism (including stroke) in the presence of thrombus is between 7% and 16% in the first few years after the event, with an annualized risk of 3.7% compared to 0.8% in patients without left ventricular thrombus. Other relevant complications include major adverse cardiovascular events (MACE), which include death, reinfarction, and hospitalization for heart failure. The presence of left ventricular thrombus is associated with a significant increase in mortality and long-term adverse cardiovascular events. In addition, patients with persistent thrombus are at increased risk of bleeding, especially if they require prolonged anticoagulation. The American Heart Association emphasizes that complete thrombus resolution is associated with lower mortality, while thrombus persistence, especially if mural and organized, carries a lower but not zero risk of embolization. The patient groups with the highest incidence of complications associated with thrombi in the left ventricle are mainly those with extensive acute myocardial infarction (AMI), especially anterior AMI, patients with ventricular aneurysm, and those with reduced left ventricular ejection fraction (LVEF). In addition, patients with dilated cardiomyopathy, either ischemic or non-ischemic, particularly those with severe systolic dysfunction, also have an elevated risk of embolic complications and major cardiovascular events. In the context of non-ischemic cardiomyopathy, patients with dilated cardiomyopathy show an even higher risk of systemic embolism compared to other non-ischemic etiologies and ischemic heart disease. The presence of mobile or protruding thrombi increases the risk of embolization, while thrombus persistence is associated with higher mortality and adverse events. The American Heart Association points out that the combination of anterior AMI, low LVEF, ventricular aneurysm, and delayed reperfusion are factors that identify patients at higher risk of embolic complications and mortality associated with thrombi in the left ventricle. The factors that increase the risk of thrombus formation in the left ventricle vary depending on the patient group, but they share pathophysiological mechanisms based on Virchow’s triad: ventricular dysfunction (stasis), endocardial damage, and inflammation/hypercoagulability. In patients with extensive acute myocardial infarction (AMI), especially anterior AMI, the highest risk factors are anterior location of the infarction, presence of ventricular aneurysm, left ventricular ejection fraction (LVEF) <30-40%, larger infarction size (elevated troponins), delayed reperfusion, and suboptimal coronary flow after intervention. The combination of reduced LVEF and segmental dysfunction (particularly apical) is the main predictor of thrombus and embolic complications or major cardiovascular events in all these groups. Systemic inflammation (elevated CRP) and the use of certain antithrombotic drugs may also contribute
Managment Management of left Heart Thrombi (RHT) The cornrstone of managment for intracardiac thrombus, particularly left ventricular thrombus, is therapeutic anticoagulantion. This strategy aims to reduce the risk of systemic embolism and promote trhombus resolution. Anticoagulation should be initiated promptly upon diagnosis, typically with intravenous unfractionated heparin, low molecular weight heparin, or a direct oral anticoagulant (DOAC). Transition to oral therapy with either warfarin or a DOAC is the recommended available evidence suggests that anticoagulation significantly lowers embolic risk and increases the likelihood of thrombus resolution compared to no or subtherapeutic treatment. In particular, a higher time in therapeutic range with warfarin is associated with superior outcomes and appears to outweigh the bleeding risks, even in the presence of concurrent antiplatelet therapy. The standard duration of anticoagulation is a minimum of three months.
Follow-up cardiac imaging, ideally using the same modality employed at diagnosis, should be performed at that point to assess thrombus resolution. If the thrombus persists without notable change, anticoagulation should be continued with periodic reassessment. In cases where the thrombus has decreased in size or displays features consistent with chronicity and reduced embolic potential, the decision to continue therapy should be based on ongoing embolic risk, such as persistent left ventricular dysfunction, aneurysm formation, or spontaneous echocardiographic contrast. If both the thrombus and contributing risk factors have resolved, evidenced by normalization of systolic function and absence of additional indications for anticoagulation, discontinuation of therapy may be appropriate. For patients who develop LVT in the context of prior MI (≥3 months) or chronic ischemic cardiomyopathy, no randomized controlled data exist to guide treatment duration. Nonetheless, anticoagulation for a period of 3 to 6 months is generally recommended. Beyond that, extended or indefinite therapy should be considered on a case-by-case basis, incorporating individual thrombotic and bleeding risks, recovery of ventricular function, and patient preferences through shared decision- making.
Management of Right Heart Thrombi (RHT) Right heart thrombi (RHT) are rare but potentially life-threatening findings, often associated with pulmonary embolism (PE) and right ventricular dysfunction. The management of RHT remains a clinical challenge due to the lack of randomized controlled trials and standardized treatment guidelines. However, observational studies and registry data suggest that anticoagulation alone is often insufficient, especially in cases involving mobile or serpiginous thrombi with high embolic potential. Initial management typically includes systemic anticoagulation with intravenous unfractionated heparin or low molecular weight heparin. This serves as a bridge to definitive therapy and may be appropriate in hemodynamically stable patients with non-mobile thrombi or contraindications to more aggressive interventions. For patients with mobile RHT or hemodynamic compromise, reperfusion strategies are generally preferred. Systemic thrombolysis has demonstrated lower mortality rates compared to anticoagulation alone, but carries a notable risk of major bleeding, including intracranial hemorrhage. Surgical embolectomy is another option, particularly in patients with contraindications to thrombolysis or when thrombi are large, organized, or entangled in cardiac structures. Catheter-directed therapies, including percutaneous aspiration thrombectomy (e.g., AngioVac, FlowTriever, AlphaVac), have gained attention as minimally invasive alternatives. These techniques allow for rapid thrombus removal with high success rates and a lower bleeding profile compared to systemic thrombolysis. Early outcomes are promising, although data remain limited and long-term efficacy has not been firmly established. Ultimately, the choice of therapy should be guided by thrombus characteristics (size, mobility, morphology), patient stability, comorbidities, bleeding risk, and institutional expertise. In general, mobile RHTs or those associated with acute PE warrant urgent intervention beyond anticoagulation alone. Multidisciplinary decision making often involving cardiology, critical care, interventional radiology, and cardiothoracic surgery is essential for optimizing outcomes.
Prevention Intracardiac thrombus formation is a recognized complication in patients with heart failure and reduced ejection fraction, particularly in those with non-ischemic dilated cardiomyopathy (DCM). Although left ventricular (LV) thrombi are more frequently documented, thrombi may also develop in the right heart chambers, especially in the presence of right-sided dysfunction, central venous catheters, cardiac devices, or systemic hypercoagulable states. The use of antithrombotic therapy for primary prevention of thrombus formation in this population remains a subject of ongoing clinical judgment. In patients with DCM who are in sinus rhythm and without prior thromboembolic events, neither aspirin nor warfarin has consistently demonstrated clear benefit in preventing thrombus formation or reducing major adverse cardiovascular events. Therefore, routine prophylactic use of these agents is generally not recommended. However, individualized assessment is essential, especially when additional risk factors such as atrial fibrillation, prior embolic events, severely reduced ejection fraction, or left ventricular aneurysms are present. In select subtypes of DCM that carry a higher inherent risk of intracardiac thrombus such as Takotsubo syndrome with apical ballooning, left ventricular noncompaction, peripartum cardiomyopathy, eosinophilic myocarditis, and infiltrative diseases like cardiac amyloidosis the use of oral anticoagulants (e.g., warfarin) or parenteral agents may be considered on a case-by-case basis. In contrast, low-dose aspirin may offer some theoretical antiplatelet benefit, but its role in thrombus prevention remains less defined. Long-term anticoagulation may be appropriate for patients with persistent ventricular dysfunction or recurrent thromboembolic risk, provided the bleeding risk is acceptable.
Bibliografia link Mathevosian, S., & Ranade, M. (2022). Right Heart Clot-in-Transit: Endovascular Therapies. Seminars in interventional radiology, 39(5), 515–522. https://doi.org/10.1055/s-0042-1757942 Sakellariou, X. M., Efstathopoulos, A., Stamatis, K. V., Nikas, D. N., & Kolettis, T. M. (2020). Treatment of Mobile Right Heart Thrombi. European journal of case reports in internal medicine, 7(12), 001918. https://doi.org/10.12890/2020_001918 Patel, A. N., Amrutiya, R. J., Manvar, B. N., & Patel, A. (2022). A proposed approach for the management of clot-in-transit. Cureus, 14(8). Lawrence LK Leung, M. D. (2025). Overview of hemostasis. https://shorturl.at/hkxsH Levine, G. N., McEvoy, J. W., Fang, J. C., Ibeh, C., McCarthy, C. P., Misra, A., Shah, Z. I., Shenoy, C., Spinler, S. A., Vallurupalli, S., Lip, G. Y. H., on behalf of the American Heart Association Council on Clinical Cardiology, Council on Cardiovascular and Stroke Nursing, & and, S. C. (2022). Management of patients at risk for and with left ventricular thrombus: A scientific statement from the american heart association. Circulation, 146(15), e205–e223. 10.1161/CIR.0000000000001092 Warren J Manning, M. D. (2024). Echocardiography in detection of cardiac and aortic sources of systemic embolism. https://shorturl.at/mR7gN Watson, N. W., Weinberg, I., Dicks, A. B., Carroll, B. J., & Secemsky, E. A. (2024). Clinical outcomes and predictors of advanced therapy for the management of right heart thrombus. Circulation: Cardiovascular Interventions, 17(4), e013637. 10.1161/CIRCINTERVENTIONS.123.013637
Wilson S Colucci, M. D., & Gregory YH Lip, MD, FRCPE, FESC, FACC. (2025). Left ventricular thrombus. https://shorturl.at/Zf9oO Kleindorfer, D. O., Towfighi, A., Chaturvedi, S., Cockroft, K. M., Gutierrez, J., Lombardi-Hill, D., Kamel, H., Kernan, W. N., Kittner, S. J., Leira, E. C., Lennon, O., Meschia, J. F., Nguyen, T. N., Pollak, P. M., Santangeli, P., Sharrief, A. Z., Smith, S. C., Jr, Turan, T. N., & Williams, L. S. (2021). 2021 guideline for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline from the American heart association/American stroke association. Stroke; a Journal of Cerebral Circulation, 52(7), e364–e467. https://doi.org/10.1161/STR.0000000000000375 Levine, G. N., McEvoy, J. W., Fang, J. C., Ibeh, C., McCarthy, C. P., Misra, A., Shah, Z. I., Shenoy, C., Spinler, S. A., Vallurupalli, S., Lip, G. Y. H., & American Heart Association Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; and Stroke Council. (2022). Management of patients at risk for and with left ventricular thrombus: A scientific statement from the American Heart Association. Circulation, 146(15), e205–e223. https://doi.org/10.1161/CIR.0000000000001092 Camaj, A., Fuster, V., Giustino, G., Bienstock, S. W., Sternheim, D., Mehran, R., Dangas, G. D., Kini, A., Sharma, S. K., Halperin, J., Dweck, M. R., & Goldman, M. E. (2022). Left ventricular thrombus following acute myocardial infarction: JACC state-of-the-art review. Journal of the American College of Cardiology, 79(10), 1010–1022. https://doi.org/10.1016/j.jacc.2022.01.011
Sharma, N. D., McCullough, P. A., Philbin, E. F., & Weaver, W. D. (2000). Left ventricular thrombus and subsequent thromboembolism in patients with severe systolic dysfunction. Chest, 117(2), 314–320. https://doi.org/10.1378/chest.117.2.314 Ram, P., Shah, M., Sirinvaravong, N., Lo, K. B., Patil, S., Patel, B., Tripathi, B., Garg, L., & Figueredo, V. (2018). Left ventricular thrombosis in acute anterior myocardial infarction: Evaluation of hospital mortality, thromboembolism, and bleeding. Clinical Cardiology, 41(10), 1289–1296. https://doi.org/10.1002/clc.23039 Albaeni, A., Chatila, K., Beydoun, H. A., Beydoun, M. A., Morsy, M., & Khalife, W. I. (2020). In-hospital left ventricular thrombus following ST-elevation myocardial infarction. International Journal of Cardiology, 299, 1–6. https://doi.org/10.1016/j.ijcard.2019.07.070
Dr. Pakeeza Saif King Edward Medical College, Lahore, Pakistan
Amin H. Karim MD Houston Methodist Academic Institute and Weill Medical College of
Dear Dentist: My Murmur Doesn’t Need Meds Anymore!
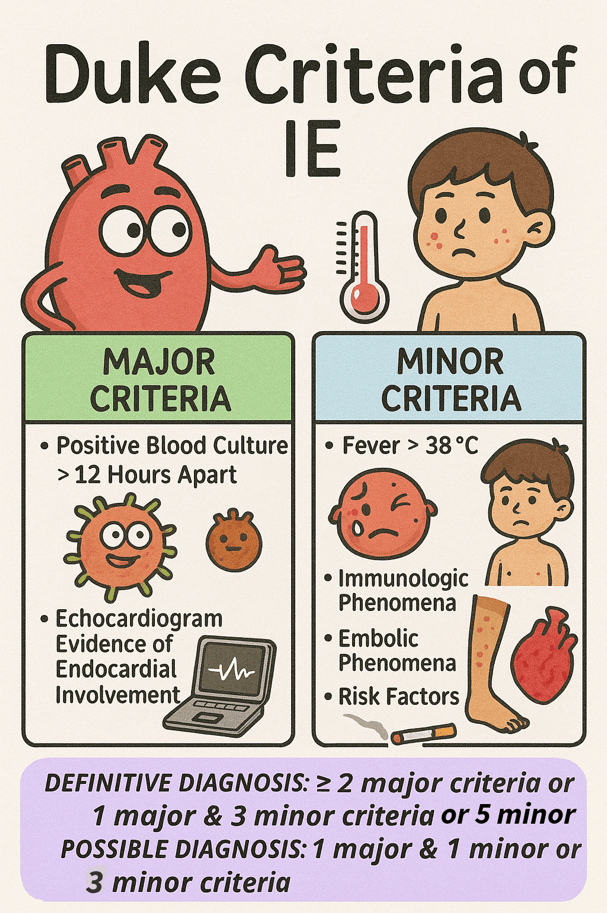
Infective endocarditis (IE) is a serious infection of the heart’s inner lining, affecting 3 to 10 people per 100,000 annually. It carries a significant risk, with mortality reaching up to 30% within the first 30 days 1 . Staphylococcus aureus was the most frequently identified pathogen, accounting for 31% of cases. The mitral valve was the most commonly affected, involved in forty-one percent of infections, while the aortic valve was affected in thirty-eight percent of cases 2. The diagnosis of IE is primarily clinical and is based on the modified Duke criteria, which include a combination of major and minor clinical, microbiological, and echocardiographic findings.
Guntheroth et al. observed that bacteremia was present in 40% of 2,403 cases following tooth extraction, 38% of individuals during routine mastication, and 11% of those with oral sepsis in the absence of any dental intervention 3. This issue has long concerned both dentists and cardiologists, driven in part by a preference for commission bias—favoring action over inaction—when considering prophylactic antibiotic use.
American Heart Association revised the guidelines on infective endocarditis prophylaxis in 2007 (full guidelines available at http://circ.ahajournals.org ) to promote the judicious use of antibiotics, particularly in clinical scenarios where the anticipated benefits are outweighed by the risks, such as the emergence of antibiotic resistance and the potential for adverse drug reactions. The present revised document was not based on the results of a single study but rather on the collective body of evidence published in numerous studies over the past two decades. The following points were used as a rationale by AHA for updating the guideline4.
IE is much more likely to result from frequent exposure to random bacteremia associated with daily activities such as chewing food, tooth brushing, flossing, use of toothpicks, use of water irrigation devices, and other activities than from bacteremia caused by a dental, gastrointestinal (GI) tract or genitourinary (GU) tract procedure.
Prophylaxis prevents only an exceedingly small number of cases of IE, if any, in individuals who undergo a dental, GI tract, or GU tract procedure.
The risk of antibiotic-associated adverse events exceeds the benefit, if any, from prophylactic antibiotic therapy except in very high-risk situations.
Maintenance of optimal oral health and hygiene may reduce the incidence of bacteremia from daily activities and thus the risk of IE and is more important than the use of prophylactic antibiotics for dental procedures 4.
Several studies have demonstrated that the lifetime risk of infective endocarditis (IE) varies significantly depending on the underlying cardiac condition. In the general population without known heart disease, the risk is approximately 5 cases per 100,000 patient-years. Patients with rheumatic heart disease (RHD) face a substantially higher risk, ranging from 380 to 440 cases per 100,000 patient-years, which is comparable to the risk observed in individuals with mechanical or bioprosthetic heart valves (308 to 383 cases per 100,000 patient-years)5 .
The greatest risks are observed in the following groups:
630 cases per 100,000 patient-years following cardiac valve replacement for native valve IE
740 cases per 100,000 patient-years in patients with a history of previous IE
2,160 cases per 100,000 patient-years in patients undergoing prosthetic valve replacement due to prosthetic valve endocarditis
These variations in risk highlight the importance of tailoring preventive measures to individual patient profiles.
Further research indicates that even with perfect effectiveness, antibiotic prophylaxis would prevent only a negligible number of infective endocarditis cases—given that the estimated absolute risk after a dental procedure is about 1 in 1.1 million for mitral valve prolapse, 1 in 475 000 for congenital heart disease, 1 in 142 000 for rheumatic heart disease, 1 in 114 000 for prosthetic heart valves, and 1 in 95 000 for those with a history of endocarditis67 .
Cardiac Conditions Associated with the Highest Risk of Adverse Outcome from Endocarditis for Which Prophylaxis Is Reasonable
Prosthetic cardiac valve or prosthetic material used for cardiac valve repair
Previous Infective Endocarditis
Cardiac transplantation recipients who develop cardiac valvulopathy
Congenital heart disease (CHD)
Unrepaired cyanotic CHD, including palliative shunts and conduits
Completely repaired congenital heart defect with prosthetic material or device, whether placed by surgery or by catheter intervention, during the first 6 months after the procedure
Repaired CHD with residual defects at the site or adjacent to the site of a prosthetic patch or prosthetic device.
Guidelines also clearly stated that antibiotic prophylaxis is no longer recommended for any other form of congenital heart disease which explicitly includesheart murmurs, valvular regurgitation, or stenosis without prosthetic material or prior endocarditis 4.
Dental procedures that involve manipulation of gingival tissue or the periapical region of teeth or perforation of the oral mucosa
Respiratory tract procedure with incision and biopsy such as tonsillectomy and adenoidectomy
Gastrointestinal or genitourinary procedures in setting of active infection
Surgery on infected skin, skin structure, or musculoskeletal tissue
Low-Risk Procedures Not Requiring Antibiotic Prophylaxis
Gastrointestinal or Genitourinary procedure in the absence of infection
Most Vaginal deliveries or Caesarian deliveries
Left atrial appendage occlusion device placement (e.g., Watchman) in the absence of infection — associated with a very low incidence of infective endocarditis, with long-term studies showing no device-related infections over extended follow-up. A single center, 14 year study of 181 patients found no device-related infections over more than 500 patient years of follow up8 .
Stable cardiac implantable electronic devices (CIEDs) such as pacemakers and ICDs — antibiotic prophylaxis is not recommended for dental or mucosal procedures solely due to the presence of a CIED in the absence of other high-risk cardiac conditions9 .
Atrial septal defect (ASD) closure devices beyond 6 months post-implantation — prophylaxis is not indicated once the device is fully endothelialized and no residual shunt remains10 .
First line: 2 g amoxicillin orally (or 50 mg/kg kids) 30–60 minutes before the procedure.
If allergic to penicillin, 600 mg clindamycin orally (or 20 mg/kg kids).
Alternatives include 500 mg azithromycin or clarithromycin orally (15 mg/kg kids)
If you can’t take pills, get 2 g ampicillin IM/IV (or 50 mg/kg kids)
Considering rising antimicrobial resistance and the potential for Clostridioides difficile infection linked to antibiotic use, it is advised against relying on the outdated “better safe than sorry” approach to prophylactic antibiotic use, as it may cause more harm than benefit to patients.
References
1. Mostaghim AS, Lo HYA, Khardori N. A retrospective epidemiologic study to define risk factors, microbiology, and clinical outcomes of infective endocarditis in a large tertiary-care teaching hospital. SAGE Open Med. 2017;5. doi:10.1177/2050312117741772
2. Murdoch DR. Clinical Presentation, Etiology, and Outcome of Infective Endocarditis in the 21st Century. Arch Intern Med. 2009;169(5):463. doi:10.1001/archinternmed.2008.603
3. Guntheroth WG. How important are dental procedures as a cause of infective endocarditis? Am J Cardiol. 1984;54(7):797-801. doi:10.1016/S0002-9149(84)80211-8
4. Wilson W, Taubert KA, Gewitz M, et al. Prevention of Infective Endocarditis. Circulation. 2007;116(15):1736-1754. doi:10.1161/CIRCULATIONAHA.106.183095
5. Steckelberg JM; WWR. Risk factors for infective endocarditis. Infectious disease clinics of North America. 1993;7(1):9-19.
6. Pallasch TJ, Wahl MJ. Focal infection: new age or ancient history? Endod Topics. 2003;4(1):32-45. doi:10.1034/j.1601-1546.2003.00002.x
7. Pallasch TJ. Antibiotic prophylaxis: problems in paradise. Dent Clin North Am. 2003;47(4):665-679. doi:10.1016/S0011-8532(03)00037-5
8. Ward RC, McGill T, Adel F, et al. Infection Rate and Outcomes of Watchman Devices: Results from a Single-Center 14-Year Experience. Biomed Hub. 2021;6(2):59-62. doi:10.1159/000516400
9. Canpolat U. Tailored antibiotic prophylaxis in patients undergoing CIED implantation: One size does not fit all the principle. Pacing and Clinical Electrophysiology. 2019;42(4):483-483. doi:10.1111/pace.13624
10. Tanabe Y, Sato Y, Izumo M, et al. Endothelialization of an Amplatzer Septal Occluder Device 6 Months Post Implantation: Is This Enough Time? An In Vivo Angioscopic Assessment. Journal of Invasive Cardiology. 2019;31(2). doi:10.25270/jic/18.00206
By Laura Edith Chavez Salas Universidad De Durango, Campus Zacatecas, Mexico
Amin H. Karim, MD Houston Methodist Academic Institute
Low-density lipoprotein (LDL) represents a category of lipoprotein particles responsible for the transport of cholesterol and various lipids within the bloodstream. Often referred to as the “bad” cholesterol, it serves vital purposes. LDL particles serve as the primary carriers of cholesterol to peripheral tissues and consist of cholesteryl esters and triglycerides encased in a phospholipid shell, free cholesterol, and a single molecule of apolipoprotein B-100. Increased levels of LDL are directly associated with the onset of atherosclerotic cardiovascular disease (ASCVD), as LDL particles can penetrate the arterial wall, become retained and altered (for instance, oxidized), and facilitate the development of foam cells and atherosclerotic plaques. (1-4)
LDL exhibits heterogeneity, with subclasses that vary in size and density; smaller, denser LDL particles are deemed more atherogenic compared to their larger, more buoyant counterparts. (3, 5, 6) The cholesterol content within LDL particles is quantified as LDL cholesterol (LDL-C), which serves as a conventional marker for evaluating and managing cardiovascular risk. (7) Nevertheless, the quantity of LDL particles (LDL-P) and the concentration of apolipoprotein B (apoB) may offer further risk stratification, particularly in individuals with metabolic syndrome or diabetes, as discrepancies between LDL-C and LDL-P can arise. (8) Evaluation of ASCVD risk can be evaluated by assessing both LDL-C and LDL-P, asserting that the reduction of LDL—primarily through the use of statins and other lipid-lowering treatments—leads to a decrease in cardiovascular events. (4)
DANGERS OF VERY LOW LDL
However, an LDL-lowering regimen can lead to ultra-low-density lipoprotein cholesterol (LDL-C) levels. These are typically defined as <40–50 mg/dL, and especially <30 mg/dL. These levels are generally well tolerated and associated with a reduced risk of atherosclerotic cardiovascular disease (ASCVD), but several potential dangers have been identified. (9) Mechanistically, very low LDL-C may impair endothelial integrity and platelet function. This could potentially increase bleeding risk, especially for intracranial and gastrointestinal hemorrhage. (10, 11)
The most observed danger of ultra-low LDL is a possible hemorrhagic stroke and other bleeding events, particularly at LDL-C levels below 40 mg/dL, as supported by mechanistic and clinical data. Observational studies and meta-analyses have also reported a U-shaped relationship between LDL-C and all-cause mortality, with both very low (<50 mg/dL) and high (≥130 mg/dL) LDL-C levels associated with increased mortality in certain populations, such as those with coronary artery disease. (15)
There is also some evidence suggesting a potential association between ultra-low LDL-C and increased risk of new-onset diabetes mellitus, particularly with statin therapy. Leading to more complications, there is a possible link to cataract formation and glaucoma, though causality remains unproven and the absolute risk is low. (11, 14)
The main dangers of ultra-low LDL-C are a possible increased risk of hemorrhagic stroke, new-onset diabetes, and, less consistently, all-cause mortality in specific populations. However, for most high-risk patients, the cardiovascular benefits of aggressive LDL-C lowering outweigh these potential risks. (9-14)
HIGH-RISK PATIENTS
Patients at highest risk for complications associated with very low levels of low-density lipoprotein cholesterol (LDL-C) are:
• Individuals with a prior history of hemorrhagic stroke:
The American Stroke Association notes that the risk of hemorrhagic stroke with statin therapy is small and nonsignificant in those without prior cerebrovascular disease, but patients with a history of hemorrhagic stroke may be at increased risk, and lipid lowering in this group requires individualized consideration and further study. (16)
• Patients with poorly controlled hypertension and very low LDL-C:
There is literature that indicates that the combination of very low LDL-C (especially ≤40 mg/dL) and uncontrolled hypertension substantially increases the risk of both ischemic and hemorrhagic stroke. Although this risk is particularly more prevalent in East Asian populations, it is relevant globally. (17)
• Women with LDL-C <70 mg/dL:
There is evidence from long-term cohort studies in women that has shown that LDL-C <70 mg/dL is associated with a more than twofold increased risk of hemorrhagic stroke compared to LDL-C 100–129.9 mg/dL, independent of other risk factors. Meaning that women with no other risk factors have more risk than males with no other risk factors. (18)
• Patients on intensive statin therapy or with other risk factors for diabetes: Statin therapy, especially at high intensity, is associated with a modestly increased risk of new-onset diabetes. Particularly in those with predisposing factors such as metabolic syndrome or impaired fasting glucose. (11)
Risks associated with having ultra-low LDL-C are more prevalent in populations most at risk, which are those with prior hemorrhagic stroke, poorly controlled hypertension, women, and individuals with multiple vascular risk factors or on intensive lipid-lowering therapy.
REFERENCES
Orlova, E V et al. “Three-dimensional structure of low density lipoproteins by electron cryomicroscopy.” Proceedings of the National Academy of Sciences of the United States of America vol. 96,15 (1999): 8420-5. doi:10.1073/pnas.96.15.8420
Rhainds, D, and L Brissette. “Low density lipoprotein uptake: holoparticle and cholesteryl ester selective uptake.” The international journal of biochemistry & cell biology vol. 31,9 (1999): 915-31. doi:10.1016/s1357-2725(99)00046-1
Qiao, Ya-Nan et al. “Low-density lipoprotein particles in atherosclerosis.” Frontiers in physiology vol. 13 931931. 30 Aug. 2022, doi:10.3389/fphys.2022.931931
Maurya, Rupesh et al. “Low density lipoprotein receptor endocytosis in cardiovascular disease and the factors affecting LDL levels.” Progress in molecular biology and translational science vol. 194 (2023): 333-345. doi:10.1016/bs.pmbts.2022.09.010
Ivanova, Ekaterina A et al. “Small Dense Low-Density Lipoprotein as Biomarker for Atherosclerotic Diseases.” Oxidative medicine and cellular longevity vol. 2017 (2017): 1273042. doi:10.1155/2017/1273042
Packard, C et al. “The role of small, dense low density lipoprotein (LDL): a new look.” International journal of cardiology vol. 74 Suppl 1 (2000): S17-22. doi:10.1016/s0167-5273(99)00107-2
Jialal, I, and A T Remaley. “Measurement of low-density lipoprotein cholesterol in assessment and management of cardiovascular disease risk.” Clinical pharmacology and therapeutics vol. 96,1 (2014): 20-2. doi:10.1038/clpt.2014.69
Galimberti, Federica et al. “Apolipoprotein B compared with low-density lipoprotein cholesterol in the atherosclerotic cardiovascular diseases risk assessment.” Pharmacological research vol. 195 (2023): 106873. doi:10.1016/j.phrs.2023.106873
Karagiannis, Angelos D et al. “How low is safe? The frontier of very low (<30 mg/dL) LDL cholesterol.” European heart journal vol. 42,22 (2021): 2154-2169. doi:10.1093/eurheartj/ehaa1080
Siniscalchi, Carmine et al. “Low LDL-Cholesterol and Hemorrhagic Risk: Mechanistic Insights and Clinical Perspectives.” International journal of molecular sciences vol. 26,12 5612. 11 Jun. 2025, doi:10.3390/ijms26125612
Cure, Erkan, and Medine Cumhur Cure. “Emerging risks of lipid-lowering therapy and low LDL levels: implications for eye, brain, and new-onset diabetes.” Lipids in health and disease vol. 24,1 185. 21 May. 2025, doi:10.1186/s12944-025-02606-6
Olsson, A G et al. “Can LDL cholesterol be too low? Possible risks of extremely low levels.” Journal of internal medicine vol. 281,6 (2017): 534-553. doi:10.1111/joim.12614
Rong, Shuang et al. “Association of Low-Density Lipoprotein Cholesterol Levels with More than 20-Year Risk of Cardiovascular and All-Cause Mortality in the General Population.” Journal of the American Heart Association vol. 11,15 (2022): e023690. doi:10.1161/JAHA.121.023690
Faselis, Charles et al. “Is very low LDL-C harmful?.” Current pharmaceutical design vol. 24,31 (2018): 3658-3664. doi:10.2174/1381612824666181008110643
Scudeler, Thiago Luis et al. “Association between low-density lipoprotein cholesterol levels and all-cause mortality in patients with coronary artery disease: a real-world analysis using data from an international network.” Scientific reports vol. 14,1 29201. 25 Nov. 2024, doi:10.1038/s41598-024-80578-w
Goldstein, Larry B., et al. “Aggressive LDL-C Lowering and the Brain: Impact on Risk for Dementia and Hemorrhagic Stroke: A Scientific Statement From the American Heart Association.” Arteriosclerosis Thrombosis and Vascular Biology, vol. 43, no. 10, Sept. 2023, https://doi.org/10.1161/atv.0000000000000164.
Wu, Zhijun et al. “The risk of ischemic stroke and hemorrhagic stroke in Chinese adults with low-density lipoprotein cholesterol concentrations < 70 mg/dL.” BMC medicine vol. 19,1 142. 16 Jun. 2021, doi:10.1186/s12916-021-02014-4
Rist, Pamela M et al. “Lipid levels and the risk of hemorrhagic stroke among women.” Neurology vol. 92,19 (2019): e2286-e2294. doi:10.1212/WNL.0000000000007454