Please watch this video. It raises some important ethical questions regarding definition of brain death.
Can the body stay alive entirely on life support and all ancillary treatment modalities if the brain ceases to function entirely, both cortex and brain stem? It has been shown that it can. Then, where does the life of a organism reside? In the brain or in the rest of the body including heart, lungs and kidneys. Amin H. Karim MD June 21 2024
Hema Manvi Koneru, MBBS, Rajiv Gandhi Institute of Medical Sciences, Telangana, India
Divyasri Koneru, MBBS, Dr.Pinnamaneni Siddartha Institute of Medical Sciences and Research Foundation, Andhra Pradesh, India.
Amanpreet Kaur, MBBS, Government Medical College, Patiala, Punjab, India.
Amin H. Karim MD Baylor College of Medicine, Houston, Texas
Introduction
Heart failure (HF) is a prevalent and serious condition associated with substantial morbidity and mortality. Management strategies have evolved, with recent focus on sodium-glucose cotransporter 2 (SGLT2) inhibitors potentially offering novel therapeutic benefits.
SGLT2 Inhibitors in HF with Reduced Ejection Fraction (HFrEF)
Studies have demonstrated that dapagliflozin, an SGLT2 inhibitor, significantly reduces the risk of worsening HF or cardiovascular death in patients with HFrEF. (1,3) The DAPA-HF trial, a pivotal phase 3 study, enrolled patients with New York Heart Association (NYHA) class II-IV symptoms and ejection fractions ≤ 40%. Results showed a reduction in the primary outcome (composite of worsening HF or cardiovascular death) among those treated with dapagliflozin compared to placebo (HR 0.74, 95% CI 0.65-0.85). This benefit was observed regardless of diabetes status, highlighting potential glucose-independent mechanisms of action.
SGLT2 Inhibitors in HF with Mildly Reduced or Preserved Ejection Fraction
Emerging evidence suggests that dapagliflozin may also benefit patients with HF and preserved or mildly reduced ejection fraction (HFpEF and HFmrEF). (2) The DELIVER trial randomized patients with HF and ejection fractions > 40% to dapagliflozin or placebo. Results indicated a reduction in the composite of worsening HF or cardiovascular death with dapagliflozin (HR 0.82, 95% CI 0.73-0.92). Moreover, improvements in symptom burden were noted, supporting potential broad utility across HF phenotypes.
Mechanisms of Action
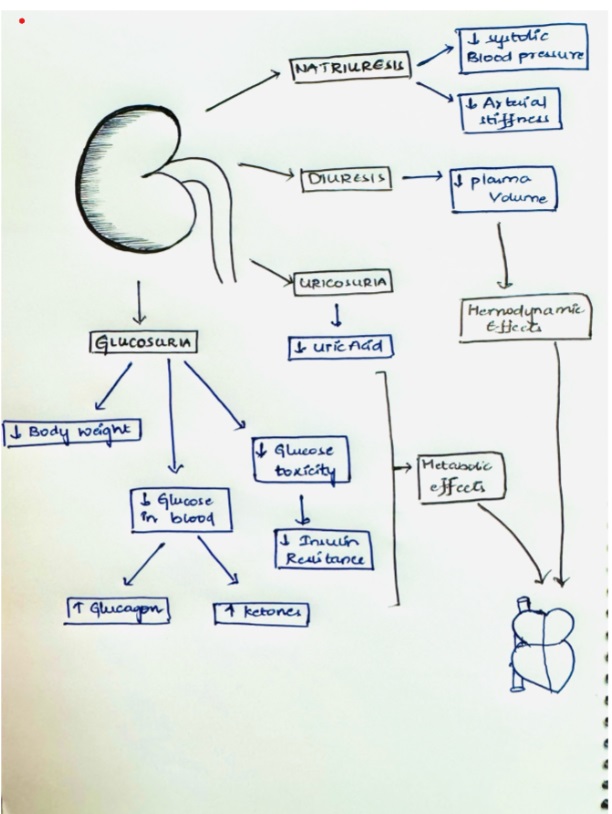
Beyond glycemic control, SGLT2 inhibitors like dapagliflozin may exert beneficial effects in HF through mechanisms including improved cardiac remodeling, reduced sodium retention, decrease plasma volume, and potential metabolic modulation. These mechanisms contribute to improved hemodynamics and reduced cardiovascular morbidity and mortality, as observed in clinical trials.
Contraindication
eGFR < 30mL/minute/1.73 m2
Safety and Tolerability
Safety profiles across trials indicate that dapagliflozin is generally well tolerated in HF patients, with adverse event rates comparable to placebo. Common side effects include volume depletion and renal dysfunction (Acute kidney injury due to dehydration), which are manageable with appropriate monitoring. Other severe side effects are euglycemic diabetic ketoacidosis, allergic reaction and genital infections (mostly fungal).
Canagliflozin increase the risk of lower limb amputation and bone fractures.
Clinical Implications and Future Directions
The efficacy of SGLT2 inhibitors in reducing HF-related events underscores their potential as adjunctive therapy in standard HF management. Future research should focus on optimizing patient selection, exploring combination therapies, and elucidating long-term benefits and risks in diverse patient populations.
Conclusion
SGLT2 inhibitors like dapagliflozin show great promise in improving outcomes for patients with heart failure. These medications not only reduce cardiovascular risks but also improve quality of life, highlighting their potential as essential elements of comprehensive heart failure treatment strategies.
References
McMurray JJV, Solomon SD, Inzucchi SE, Køber L, Kosiborod MN, Martinez FA, Ponikowski P, Sabatine MS, Anand IS, Bělohlávek J, Böhm M, Chiang CE, Chopra VK, de Boer RA, Desai AS, Diez M, Drozdz J, Dukát A, Ge J, Howlett JG, Katova T, Kitakaze M, Ljungman CEA, Merkely B, Nicolau JC, O’Meara E, Petrie MC, Vinh PN, Schou M, Tereshchenko S, Verma S, Held C, DeMets DL, Docherty KF, Jhund PS, Bengtsson O, Sjöstrand M, Langkilde AM; DAPA-HF Trial Committees and Investigators. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N Engl J Med. 2019 Nov 21;381(21):1995-2008. doi: 10.1056/NEJMoa1911303. Epub 2019 Sep 19. PMID: 31535829.
Solomon SD, McMurray JJV, Claggett B, de Boer RA, DeMets D, Hernandez AF, Inzucchi SE, Kosiborod MN, Lam CSP, Martinez F, Shah SJ, Desai AS, Jhund PS, Belohlavek J, Chiang CE, Borleffs CJW, Comin-Colet J, Dobreanu D, Drozdz J, Fang JC, Alcocer-Gamba MA, Al Habeeb W, Han Y, Cabrera Honorio JW, Janssens SP, Katova T, Kitakaze M, Merkely B, O’Meara E, Saraiva JFK, Tereshchenko SN, Thierer J, Vaduganathan M, Vardeny O, Verma S, Pham VN, Wilderäng U, Zaozerska N, Bachus E, Lindholm D, Petersson M, Langkilde AM; DELIVER Trial Committees and Investigators. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N Engl J Med. 2022 Sep 22;387(12):1089-1098. doi: 10.1056/NEJMoa2206286. Epub 2022 Aug 27. PMID: 36027570.
Nassif ME, Windsor SL, Borlaug BA, Kitzman DW, Shah SJ, Tang F, Khariton Y, Malik AO, Khumri T, Umpierrez G, Lamba S, Sharma K, Khan SS, Chandra L, Gordon RA, Ryan JJ, Chaudhry SP, Joseph SM, Chow CH, Kanwar MK, Pursley M, Siraj ES, Lewis GD, Clemson BS, Fong M, Kosiborod MN. The SGLT2 inhibitor dapagliflozin in heart failure with preserved ejection fraction: a multicenter randomized trial. Nat Med. 2021 Nov;27(11):1954-1960. doi: 10.1038/s41591-021-01536-x. Epub 2021 Oct 28. PMID: 34711976; PMCID: PMC8604725.
Petrie MC, Verma S, Docherty KF, Inzucchi SE, Anand I, Belohlávek J, Böhm M, Chiang CE, Chopra VK, de Boer RA, Desai AS, Diez M, Drozdz J, Dukát A, Ge J, Howlett J, Katova T, Kitakaze M, Ljungman CEA, Merkely B, Nicolau JC, O’Meara E, Vinh PN, Schou M, Tereshchenko S, Køber L, Kosiborod MN, Langkilde AM, Martinez FA, Ponikowski P, Sabatine MS, Sjöstrand M, Solomon SD, Johanson P, Greasley PJ, Boulton D, Bengtsson O, Jhund PS, McMurray JJV. Effect of Dapagliflozin on Worsening Heart Failure and Cardiovascular Death in Patients With Heart Failure With and Without Diabetes. JAMA. 2020 Apr 14;323(14):1353-1368. doi: 10.1001/jama.2020.1906. Erratum in: JAMA. 2021 Apr 6;325(13):1335. doi: 10.1001/jama.2021.2802. PMID: 32219386; PMCID: PMC7157181.
Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, Silverman MG, Zelniker TA, Kuder JF, Murphy SA, Bhatt DL, Leiter LA, McGuire DK, Wilding JPH, Ruff CT, Gause-Nilsson IAM, Fredriksson M, Johansson PA, Langkilde AM, Sabatine MS; DECLARE–TIMI 58 Investigators. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med. 2019 Jan 24;380(4):347-357. doi: 10.1056/NEJMoa1812389. Epub 2018 Nov 10. PMID: 30415602.
Hema Manvi Koneru, MBBS Rajiv Gandhi Institute of Medical Sciences, Telangana, India.
Amanpreet Kaur, MBBS Government Medical College Patiala, India.
Divyasri Koneru, MBBS Dr.Pinnamaneni Siddhartha Institute of Medical Sciences and Research Foundation, India
Amin H. Karim MD FACC, Clinical assistant professor, Baylor College of Medicine, Houston, Texas.
A 74-year-old male presented with complaints of dizziness. His medical history includes hypertension, diabetes mellitus, mitral regurgitation, tricuspid regurgitation, and a transient ischemic attack five months prior. Additionally, he reported two episodes of memory lapses within the past year.
The patient denied experiencing orthopnea, paroxysmal nocturnal dyspnea, chest pain, smoking, shortness of breath, leg swelling, speech disturbances, disequilibrium, blurry vision, syncope, tinnitus, hearing loss, ataxia, numbness, tingling, pins, and needles in the arms or legs.
MEDICATIONS
Aspirin 81mg sustained-release oral tablet, once daily; atorvastatin calcium 80mg tablet, taken orally once daily; clopidogrel 75mg tablet, taken orally daily; dulaglutide 0.75mg/0.5ml subcutaneous pen injector, administered subcutaneously once weekly; gabapentin 300mg oral capsule, taken once daily; losartan 25mg tablet, taken orally once daily; metformin hydrochloride 750mg extended-release tablet, taken twice daily with meals; nitroglycerin 0.4 mg sublingual tablet, to be used when chest pain persists; and thiamine 100 mg oral tablet, taken once daily. These medications have been prescribed to effectively manage the patient’s medical conditions and symptoms.
The patient had a history of allergy to the contrast medium used for the radiological examination.
LAB WORKUP
HBA1C-6.6gm/dl
The rest of the blood reports- are within in normal range.
ELECTROCARDIOGRAM
Sinus tachycardia with nonspecific ST-abnormality
CTA CORONARY ARTERIES
There is severe coronary calcification. The observed calcium score is 780, which is at the 75th percentile for subjects of the same age, gender, race/ethnicity who are free of clinical cardiovascular disease and treated diabetes.
Moderate to severe, predominantly calcified. Coronary artery disease involving proximal and LAD with moderate luminal stenosis. FFR-CT was performed on the LAD which showed significant flow limitation of the mid-LAD (left anterior descending artery).
CTA OF BRAIN AND NECK
Brain–moderate chronic microvascular ischemia, suprasellar 8 x 7 mm partially calcified lipoma or dermoid cyst.
Neck-Complete occlusion of the left vertebral artery V1 and V2 segments. Atherosclerosis of bilateral extracranial carotid arteries without significant stenosis.
The head shows no significant stenosis or occlusion.
MRI BRAIN
No acute ischemia.
Hypothalamus showing non-enhancing mass suggestive of Lipoma/Dermoid cyst.
Moderate chronic microvascular ischemia.
ECHOCARDIOGRAM
Mild left ventricular hypertrophy.
Trace tricuspid regurgitation.
Mitral regurgitation.
Left ventricular dysfunction.
NUCLEAR STRESS TEST
A small area of perfusion defect in the inferior wall which fills with reperfusion
CAROTID ULTRASOUND
No occlusive disease.
Following a thorough workup and assessment of the patient’s clinical presentation, imaging studies, and diagnostic tests, a final diagnosis of subclavian steal syndrome was made. This condition is attributed to the underlying pathology of atherosclerosis which mainly affects the subclavian artery.
DEFINITION
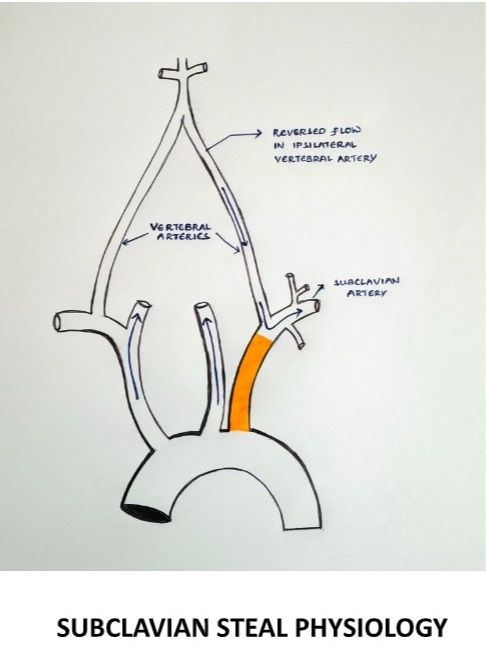
It is characterized by the retrograde flow of blood in the vertebral artery, primarily resulting from significant stenosis or occlusion in the pre-vertebral subclavian artery resulting in cerebrovascular symptoms on the ipsilateral side of the occlusion.
§ During exertion, the subclavian artery steals blood from the vertebrobasilar artery circulation to supply the arm, which leads to vertebrobasilar insufficiency.
SUBCLAVIAN STEAL PHYSIOLOGY
EPIDEMIOLOGY
The prevalence of subclavian steal syndrome has not been well defined, although subclavian steal physiology has been reported in 1.3 to 2.6% of the general population of patients with extracranial atherosclerosis (1,2) as well as within subsets of those presenting with acute ischemic stroke (3)
ETIOLOGY
The most common cause is atherosclerosis.
Other vascular causes- Takayasu arteritis, giant cell arteritis
Arterial thoracic outlet syndrome
Congenital anomalies- anomalies of the aortic arch, anomalies of the brachiocephalic trunk
A consequence of corrective surgery- surgical repair of the Tetralogy of Fallot with a Blalock-Taussig anastomosis, surgical management of the coarctation of the aorta.
Subclavian stenosis more commonly occurs on the left side (>75 percent), possibly due to more acute origin on the left subclavian artery resulting in accelerated atherosclerosis from increased turbulence. (4,5,6)
CLINICAL FEATURES
Neurovascular symptoms can be caused by vertebrobasilar ischemia of the brainstem or cerebellum
Symptoms include dizziness, vertigo, binocular double vision, dysarthria, syncope, and drop attacks (sudden falls without loss of consciousness) (7)
Episodes can be precipitated by exercise of the ischemic arm and precipitated by certain head movements.
Atypical neurological presentations- there is also increasing recognition that patients with vertebrobasilar insufficiency can present with other types of symptoms not directly attributable to brainstem or cerebellar ischemia.
Subarachnoid hemorrhage (8)
Cognitive and mood abnormalities
EVALUATION
Although neurovascular symptoms associated with subclavian steal physiology occur in only a minority of patients, symptoms of vertebrobasilar ischemia demand critical evaluation (10,11)
When to suspect subclavian steal syndrome
Diagnosis should be considered in patients with a measurable upper extremity blood pressure differential who develop episodic neurological symptoms attributable to the brainstem or cerebellar ischemia.
Suspicion is increased if the episodes are provoked by arm exercise, especially if accompanied by ischemic arm symptoms (7)
PHYSICAL EXAMINATION
All major pulses should be palpated, and blood pressure should be checked in both arms.
It is important to examine the subclavian arteries in the supraclavicular fossa using palpation and auscultation for paraventricular bruits, also vertebral and carotid arteries for the evidence of any occlusive arterial disease.
On examination, there may be a significant decrease in the blood pressure on the affected side with a pulse delay appreciated when palpating the radial arteries simultaneously known as RADIO-RADIAL DELAY.
Check for any evidence of thromboembolism in the skin of the hands and nailbeds of the affected extremities.
Ischemia affecting the temporo-occipital areas of the cerebral hemispheres or segments of the brainstem and cerebellum characteristically produces bilateral symptoms.
RADIOLOGICAL EXAMINATION
Initial vascular imaging
1. Duplex ultrasound
A subclavian artery peak systolic velocity >240cm/sec is predictive of a significant (>70 percent) subclavian artery stenosis (9)
When severe stenosis (>80 percent narrowing) of the proximal subclavian artery is present, 65 percent of pa>ents have permanent flow reversal in the ipsilateral vertebral artery, and 30 percent have intermittent flow reversal (10,11)
2. Transcranial doppler ultrasound
Confirmatory vascular imaging
Computed tomographic angiography (CTA)-provides precise measurement of the severity of the stenosis. main drawback is the absence of dynamic flow information.
Magnetic resonance angiography (MRA)- sensitive than CTA. Does not depict images of arterial anatomy but rather the behavior and speed of the flowing protons in the vessel. Also provides information on the intracranial cerebrovascular circulation.
Catheter-based digital subtraction angiography (DSA)
DIAGNOSIS
DIAGNOSTIC CRITERIA– the presence of subclavian steal physiology with demonstration of a subclavian artery stenosis/ occlusion proximal to the origin of the vertebral artery causing
Marked reduction in the ipsilateral brachial artery blood pressure.
Reversal of the direction of blood flow in the ipsilateral vertebral artery
Neurological symptoms referrable to the vertebrobasilar circulation (cerebellum, brainstem, thalamus, occipital regions)
The likelihood that the presence of subclavian steal physiology will lead to the subclavian steal syndrome increases as the brachial pressure differential between the two limbs becomes more pronounced, particularly >40mmhg (5)
DIFFERENTIAL DIAGNOSIS
These include all the potential causes of vertebrobasilar embolism due to atherosclerosis, hypertension, hypercoagulable states, tumors, tobacco smoking, trauma, and others
MANAGEMENT
Management of patients with subclavian steal syndrome is individualized depending on the etiology, type, and severity of symptoms and their impact on quality of life
ATHEROSCLEROTIC SUBCLAVIAN STEAL SYNDROMEAPPROACH
For most patients with atherosclerosis as the etiology for subclavian steal syndrome, conservative management is the preferred initial therapy.
Initial medical management
Start with the low-dose aspirin.
However, the addition of other anti-platelet drugs does not seem justified since this condition is hemodynamic derangement. once a decision is made for surgical management, additional anti-thrombotic agents are required.
Optimal blood pressure management is required within the ipsilateral side brachial artery.
Surgical management
Proximal subclavian endarterectomy, which is a trans-thoracic approach used for revascularizing the subclavian artery.
Re-vascularization surgery via endovascular techniques (carotid-subclavian bypass or subclavian-carotid transposition).
Carotid intervention in patients with severe concomitant carotid artery disease helps to improve cerebral perfusion.
NON-ATHEROSCLEROTIC SUBCLAVIAN STEAL SYNDROME
For non-atherosclerotic subclavian syndrome etiologies, the primary cause needs to be addressed.
Example- Takayasu arteritis is by systemic glucocorticoids or steroid-sparing agents like biological DMARD (Disease Modifying Anti-Rheumatoid Drugs) or non-biological DMARD
CONCLUSION
This case highlights the importance of a detailed evaluation of subclavian steal syndrome can be due to atherosclerosis or non-atherosclerotic causes like Takayasu arteritis, giant cell arteritis, arterial thoracic outlet syndrome, and other causes. In our case, it might be a subclavian steal syndrome secondary to atherosclerosis.
REFERENCES
Fields WS, Lemak NA. Joint Study of extracranial arterial occlusion. VII. Subclavian steal–a review of 168 cases. JAMA. 1972 Nov 27;222(9):1139-43. PMID: 4678043.
Hennerici M, Klemm C, Rautenberg W. The subclavian steal phenomenon: a common vascular disorder with rare neurologic deficits. Neurology. 1988 May;38(5):669-73. doi: 10.1212/wnl.38.5.669. PMID: 3362359.
Bajko Z, Motataianu A, Stoian A, Barcutean L, Andone S, Maier S, Drăghici IA, Cioban A, Balasa R. Prevalence and Clinical Characteristics of Subclavian Steal Phenomenon/Syndrome in Patients with Acute Ischemic Stroke. J Clin Med. 2021 Nov 10;10(22):5237. doi: 10.3390/jcm10225237. PMID: 34830519; PMCID: PMC8621575.
Ochoa VM, Yeghiazarians Y. Subclavian artery stenosis: a review for the vascular medicine practitioner. Vasc Med. 2011 Feb;16(1):29-34. doi: 10.1177/1358863X10384174. Epub 2010 Nov 15. PMID: 21078767.
Labropoulos N, Nandivada P, Bekelis K. Prevalence and impact of the subclavian steal syndrome. Ann Surg. 2010 Jul;252(1):166-70. doi: 10.1097/SLA.0b013e3181e3375a. PMID: 20531004.
Shadman R, Criqui MH, Bundens WP, Fronek A, Denenberg JO, Gamst AC, McDermott MM. Subclavian artery stenosis: prevalence, risk factors, and association with cardiovascular diseases. J Am Coll Cardiol. 2004 Aug 4;44(3):618-23. doi: 10.1016/j.jacc.2004.04.044. PMID: 15358030.
KESTELOOT H, VANHOUTE O. REVERSED CIRCULATION THROUGH THE VERTEBRAL ARTERY. Acta Cardiol. 1963;18:285-99. PMID: 14045892.
Rodriguez-Lopez JA, Werner A, Martinez R, Torruella LJ, Ray LI, Diethrich EB. Stenting for atherosclerotic occlusive disease of the subclavian artery. Ann Vasc Surg. 1999 May;13(3):254-60. doi: 10.1007/s100169900254. PMID: 10347257.
Gutierrez GR, Mahrer P, Aharonian V, Mansukhani P, Bruss J. Prevalence of subclavian artery stenosis in patients with peripheral vascular disease. Angiology. 2001 Mar;52(3):189-94. doi: 10.1177/000331970105200305. PMID: 11269782.
Osiro S, Zurada A, Gielecki J, Shoja MM, Tubbs RS, Loukas M. A review of subclavian steal syndrome with clinical correlation. Med Sci Monit. 2012 May;18(5):RA57-63. doi: 10.12659/msm.882721. PMID: 22534720; PMCID: PMC3560638.
Cornelissen SA, Heye S, Maleux G, Daenens K, van Loon J, De Vleeschouwer S. Treatment of ruptured subclavian steal flow-related vertebrobasilar junction aneurysms: Case report on surgical and endovascular considerations from two cases. Int J Surg Case Rep. 2022 Jan;90:106744. doi: 10.1016/j.ijscr.2021.106744. Epub 2021 Dec 30. PMID: 34991048; PMCID: PMC8741505.
Ahuja CK, Joshi M, Mohindra S, Khandelwal N. Vertebrobasilar Junction Aneurysm Associated with Subclavian Steal: Yet another Hemodynamic Cause for Aneurysm Development and Associated Challenges. Neurol India. 2020 May-Jun;68(3):708-709. doi: 10.4103/0028-3886.288981. PMID: 32643699.
Tonetti DA, Jankowitz BT. Subclavian Steal Flow-Related Aneurysm Formation. World Neurosurg. 2019 May;125:101-103. doi: 10.1016/j.wneu.2019.01.186. Epub 2019 Feb 8. PMID: 30743034.
Mousa AY, Morkous R, Broce M, Yacoub M, Sticco A, Viradia R, Bates MC, AbuRahma AF. Validation of subclavian duplex velocity criteria to grade severity of subclavian artery stenosis. J Vasc Surg. 2017 Jun;65(6):1779-1785. doi: 10.1016/j.jvs.2016.12.098. Epub 2017 Feb 17. PMID: 28222983.
Nicholls SC, Koutlas TC, Strandness DE. Clinical significance of retrograde flow in the vertebral artery. Ann Vasc Surg. 1991 Jul;5(4):331-6. doi: 10.1007/BF02015293. PMID: 1878290.
Harper C, Cardullo PA, Weyman AK, Patterson RB. Transcranial Doppler ultrasonography of the basilar artery in patients with retrograde vertebral artery flow. J Vasc Surg. 2008 Oct;48(4):859-64. doi: 10.1016/j.jvs.2008.05.057. Epub 2008 Aug 9. PMID: 18692344.
From Accidents to Advancements in the Realm of Medications.
Mahmood Syed, MS4 American University School of Medicine
Amanpreet Kaur, MBBS Government Medical College Patiala, India
Amin H. Karim MD FACC Clinical Assistant Professor Baylor College of Medicine, Houston, Texas.
“When you have acquired knowledge and experience, it is very pleasant to break the rules and to be able to find something nobody has thought of.” These were the words of renowned Bacteriologist, Andrew Fleming, who discovered Penicillin widely used today. There are drugs whose original discovery was intended for specific indications. However, their side effects were so useful that these medications were eventually repurposed as treatments for other medical conditions. This phenomenon is also known as “drug repurposing” or “serendipitous discovery”. Here are some examples of such medications widely used today:
The discovery of Minoxidil is a fascinating chapter in medicinal advancements. It was initially created for the treatment of Hypertension. However, during clinical studies, scientists discovered a surprising adverse effect that caused hair growth in patients that were taking this medication. This coincidental finding prompted more research into Minoxidil’s potential as a male pattern baldness remedy. Eventually, it was repurposed for this indication.
Viagra (Sildenafil) is another interesting medication that was unintentionally found while being used in the treatment of Angina Pectoris and Pulmonary Hypertension. An unanticipated side effect that the researchers discovered during clinical trials was that many of the male participants reported having better erectile function after taking this medication due to its vasodilatory effects. Therefore, it was repurposed as a medication for men suffering from Erectile Dysfunction (ED).
Bimatoprost was another medication that was initially discovered for the treatment of Glaucoma, but researchers noted that it increased eyelash length, thickness, and blackness in the patients who received these eye drops for the treatment of Glaucoma. This led to its use for cosmetic enhancement of eyelashes today.
Ozempic (Semaglutide) was originally discovered for the treatment of Type 2 Diabetes Mellitus. This medication functioned as a GLP-1 agonist. Researchers found that it caused significant weight reduction in addition to controlling blood glucose levels. After further clinical trials, it was approved as a medication for weight loss.
Gabapentin was initially discovered as a potential treatment for seizures as it was structurally similar to the neurotransmitter GABA. After its initial discovery, Gabapentin was subsequently found to have efficacy in treating neuropathic pain in patients who were treated for seizures, leading to its approval for this indication as well.
Finasteride was initially investigated for its potential use in the treatment of Benign Prostatic Hyperplasia. While clinical trials were ongoing to see the effectiveness of this medication for BPH, it was observed that patients taking finasteride experienced hair growth as a side effect. Eventually, it was repurposed for the treatment of hair loss.
Methotrexate, a potent inhibitor of Folate metabolism, was used for the treatment of many cancers including Acute Lymphocytic Leukemia (ALL) and Choriocarcinoma. It was discovered to be effective in treating autoimmune conditions due to its ability to inhibit cell growth and modulate immune responses. Today, it is used to treat conditions like Systemic Lupus Erythematosus (SLE) and Rheumatoid Arthritis (RA).
The development of aspirin from a painkiller to a multi-indicated drug is evidence regarding its healing characteristics. Initially, aspirin was found to be useful for reducing fever and pain. However, it is now essential for maintaining cardiovascular health, controlling inflammation, and even preventing and reducing the incidence of cancer, particularly in the setting of colon cancer. This extensive range of applications highlights the significance of aspirin in modern medicine and its ongoing importance over a century after it was initially discovered.
There are other medications that produce treatment indications as a result of their side effect. In the world of ever-evolving medicine and advancements in medical research, there is no doubt there will be more discoveries of newer medications as well as current medications with newer indications. The medical field is expanding on a level never experienced before in humanity. As new therapies become available, as well as more research being generated as a result of clinical trials and controlled studies, we will see an even greater advancement in medicine in the near future than we have ever seen before. The only limitation that we have is the limitations we set on ourselves. In the book, The Laws of Medicine, by Pulitzer Prize-winning author Siddhartha Mukherjee, he says “ In medicine, mistakes are inevitable but learning from them is essential.” Furthermore, if these mistakes lead to newer discoveries and treatments in the realm of medicine, then mistakes might just be better than getting it right the first time.
It was 1981. I had finished my residency at Cook County Hospital Chicago 2 years ago & was struggling to find a private practice. Those days were rather difficult to establish a new pediatrics practice as most of the Family practice docs would take care of the kiddos. After working as part time attending physician at Cook county Hospital Chicago with moonlighting here & there, I decided to move to California. In fact a friend of mine Dr M Ashraf, who was already practicing Cardiology in Madera California, invited me to visit the town & take over a small practice which was for sale.
So 43 years ago June 1, 1981 I started my practice. It was slow going but steadily improving. One day an 11 month old girl Maria was brought it with fever & jaundice. Since Hepatitis A was common at that time in the area, I diagnosed her with it & advised routine dietary management. A week later she returned with ascites.
Her liver was failing, so I admitted her in the community hospital & initiated the workup. Her LFT,s were slightly abnormal, bilirubin was about 8 mg/dl & hemoglobin was about 10gram. All other tests were normal. Due to increasing ascites, I transferred to local Children hospital in Fresno
At the children hospital a GI fellow would come twice a month from UCSF San Francisco. He decided to transfer Maria to SFO as her ascites was worsening inspite of treatment with diuretics & whatever else they had.
At UCSF, a liver biopsy was done & found to have nonspecific inflammatory changes. In the next 3 weeks, her ascites got significantly worse. Parents were advised that she had liver failure & she was not going to make it . So they decided to bring her back home to Madera AMA as it was easier to transport a live person than a dead body.
MARIA IN MADERA
By this time about 2 months had passed & patient was really uncomfortable due to increased intra-abdominal pressure. She has persistent cough due to shortness of breath. She was brought back to my office for cough. I advised them that she needs relief of pressure from her abdomen. Parents did not want any heroic measures done as “ she is going to die anyway “. I advised them that “yes. But let her die in peace”.
I called FRESNO children hospital & UCSF & they both refused to take her in as she was terminal anyway. Our local Gastroenterologist & surgeon also had their hand up by saying they were not pediatrics specialists. I asked an old FP how to do an abdominal paracentesis & admitted her in my local hospital.
This was my FIRST & LAST abdominal tap of my life. I took out 700 CC fluid first day & another 300 CC. the next day. She was comfortable & was discharged home.
I saw her in my office a week later. Her abdominal girth was the same as at the time of discharge. A month later her abdominal girth was normal & she was an active happy toddler. At age 16 Maria had splenic infarction & had splenectomy done at our hospital. At age 18 she had her first child & after 3 children she moved out of town & got lost to follow up.
I had been a “PEER” for the family. They sent me so many patients. And my practice flourishes until now thank God. All I did was make her comfortable.
I informed the UCSF about the happy outcome and they asked me to send her back for further biopsy which I did not comply. They were not helpful when I needed them the most. Unfortunately I never thought of getting all the medical records & write it up for a journal. Now our hospital has been closed also. This story is all from my memory.
85 year old man admitted with CP in setting of HTN. Had has symptoms for a few months. ECG showed ST depression and the EF was 45%. The referring sent him for CABG but the (chief) surgeon was hesitant because the patient is a Jehovah’s witness (can not receive blood), low platelets (85k), and high Cr (1.9)
.
What is your ABC analysis? As a reminder: A – angiographic analysis, B – bifurcation strategy, C – calcium modulation, D – device (MCS) selection if any, and E – execution strategy?
Ok, so the resolution of our case…
These were my thoughts going into the case…
A. Functional last conduit because the RCA is critical. The entire body of the LM is involved. Heavy calcium is an understatement.
B. Medina 1,1,1 – both arteries need to be addressed. Our plan was to perform DK crush.
C. Rota and/or IVL. ‘Relative’ disadvantages to both – Rota will require me to remove the wire from one of the branches. IVL will prolong LM occlusion (= ischemic) time.
D. Definitely Impella supported.
E. Plan – perform RHC for reserve, insert Impella, wire both LAD and LCX, PTCA LM into LAD, IVUS then decide on rota strategy, finish with DK crush. Stage RCA.
We started by doing a RHC. The PA pressures were not too bad (48) and the PA sat was reassuring 58%. We opted for dual access.
We resolved that issue with a TurnPike LP microcatheter. You can drive the MC by torquing it. We knew we were going to fix the LAD with rota so I did a 1.5 mm angioplasty to allow the LAD to breathe while we did IVUS.
With the LAD and LCX fixed, the LM is more manageable now. We opted to finish the T-stent and use IVUS to see if further optimization was needed.Our bifurcation plan rapidly evolved during the case. It was DK crush before the case, mini crush after I put the proximal LCX stent in, and ended up being a T-stent because of how well the stent had landed at the ostium.
You can see the patient is becoming restless. I think that it was likely from leg ischemia related to the Impella sheath.
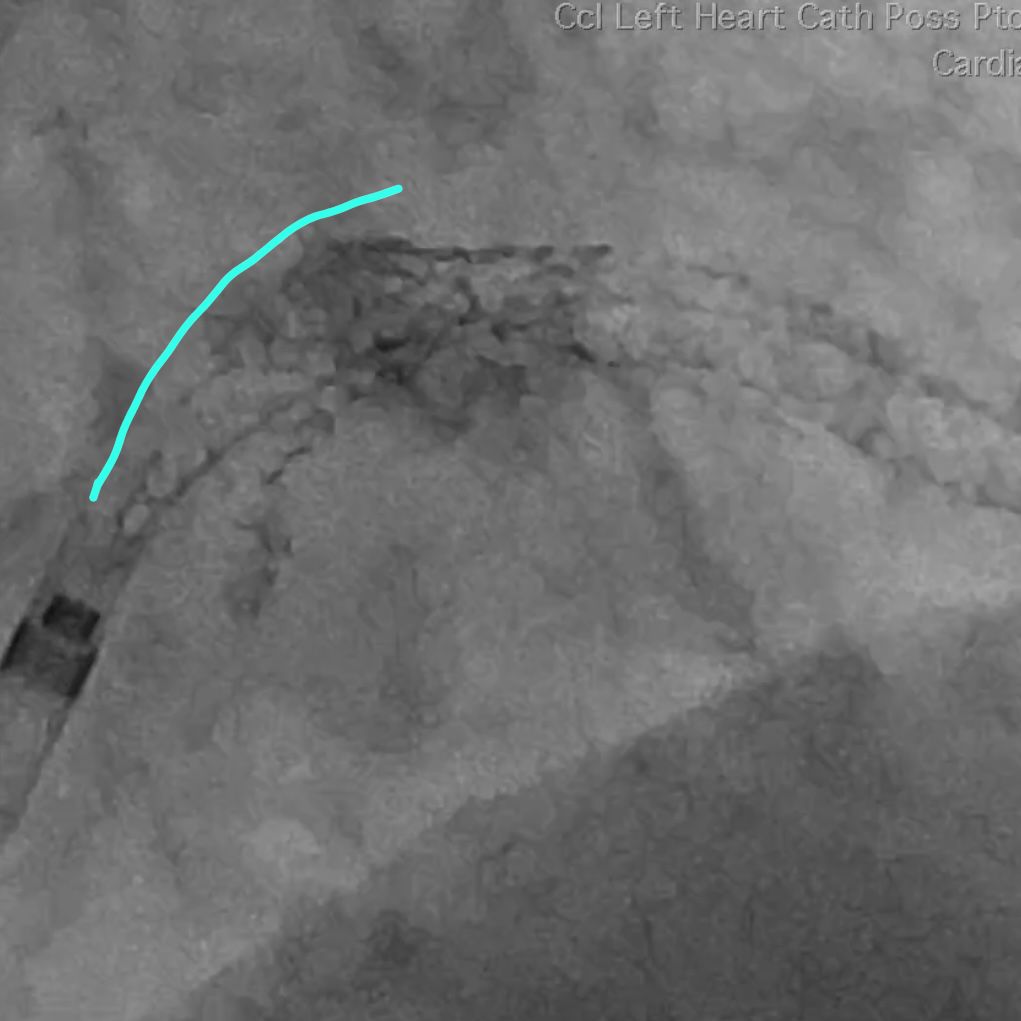
Also, the guide had softened and came out. Note the stent deformation on account of the calcium module at the ostium. There is a recoil after high-pressure NC ballooning.
Here is the CFA after Impella removal. We did not use single access because I wanted to use a 7 French guide without any of the drama. A 7 French sheath is often quite snug in the Impella insertion sheath. The double access also allowed us to ensure that the bleeding at the Impella insertion site had completely stopped before the patient left the Cath Lab. This was on on account of his inability to receive blood being a Jehovah’s witness.
The patient did very well. He was up and about the next day. He did have a mild bump in his creatinine, but we kept him for a few days.
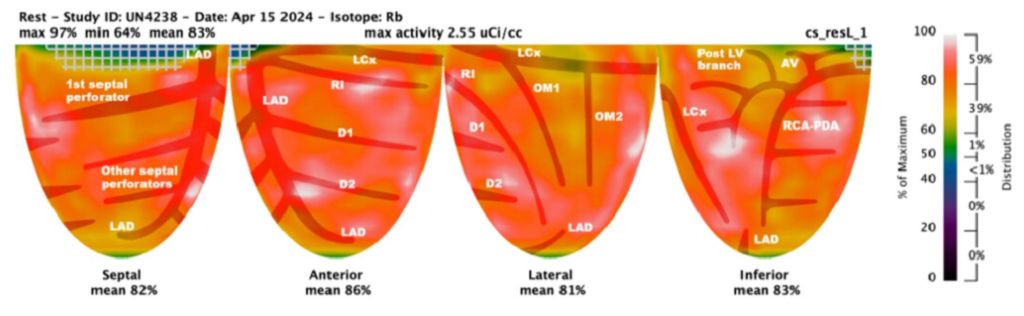
I plan to perform an PET in four weeks and then decide if he needs the RCA fixed. Again, he is an 85 year old who has been doing quite well until now.
The End. 🙏🏼
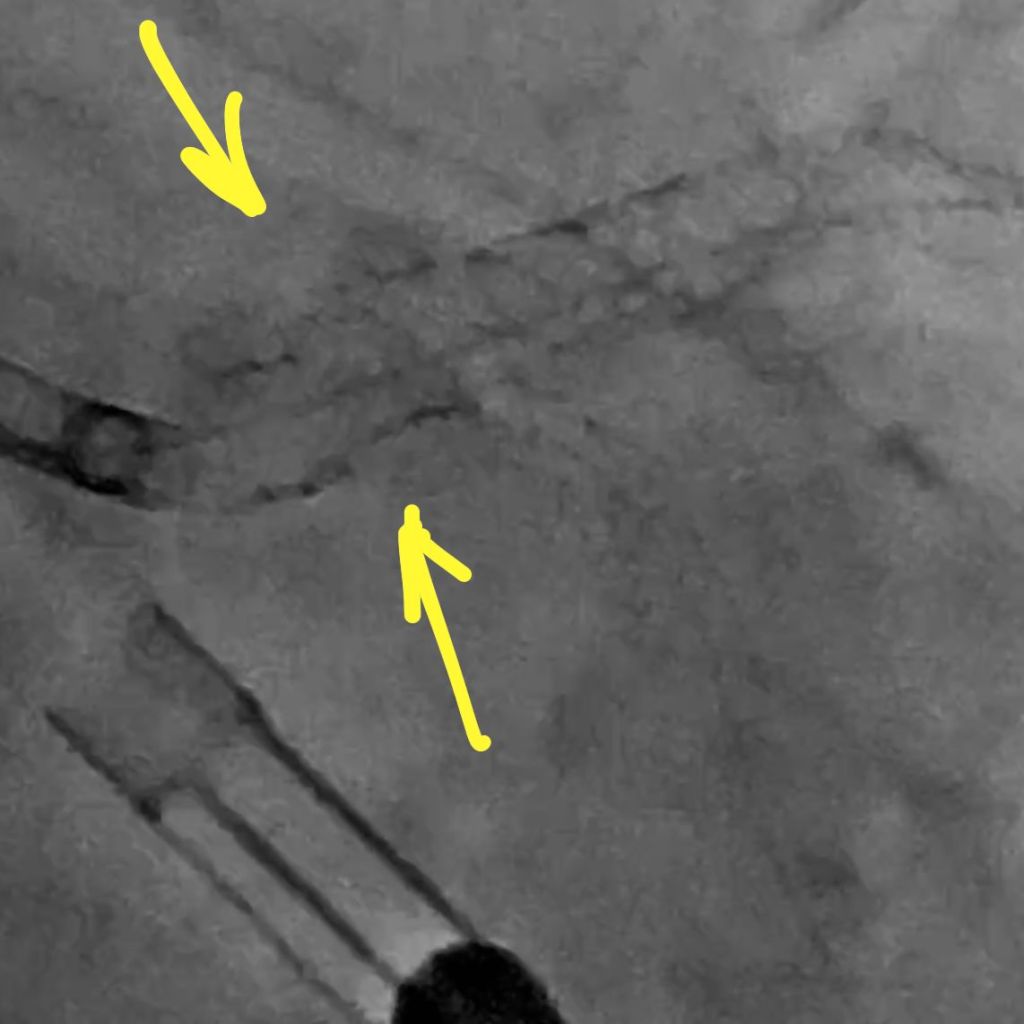
I am going to share a series of still frames that shows the changing morphology of the LM lumen. This is baseline.
Here is the balloon inflation. Note the upward displacement of the nodules.
This is after our aggressive POT. Note the smoother upper curvature.
A young man came to his internal medicine physician over several years for various symptom-focused visits. On the majority of these visits the patient’s blood pressure readings were elevated. Two months after his last exam, the patient died suddenly at home. He was 31 years of age. The cause of death was determined to be a complete occlusion of the left anterior descending artery (LAD).
Autopsy findings were inconsistent with hypertensive coronary artery disease, as there was no heart enlargement, dilation of the left ventricle, pitting of the kidney surfaces, or dilation of the aorta. The pathologist did not see any evidence of end-stage organ damage caused by untreated hypertension. The pathologist concluded that the cause of death was from atherosclerotic plaque becoming disrupted and traveling to the LAD, causing occlusion and a fatal arrhythmia.
Both the pathologist and consulting cardiologist agreed this heart attack could not have been prevented since the patient did not suffer from hypertension-induced coronary artery disease.
The defendant, while providing reasonable episodic care, did not address the patient’s elevated blood pressure. The physician says he instructed the patient to watch his diet, but this was not documented in the records. The physician did not order any lab work or evaluations addressing the hypertension.
Allegations
The patient’s family filed a lawsuit against the physician for failure to diagnose and treat hypertension. It was further alleged that the physician failed to order proper evaluations and lab work and failed to provide the patient with precautions and advice on lifestyle changes. The plaintiffs argued that had the physician treated the patient’s hypertension, it would have prevented the sudden heart attack and death.
Legal implications
The patient came to the physician nine times over an 8-year period for various symptoms. During this time the patient never described any chest pain or dyspnea that would have increased the suspicion of heart disease in such a young patient. However, high blood pressure is a risk factor for heart disease, and the patient’s initial blood pressure reading was 164/110 mm Hg. Although the blood pressure readings fluctuated, consultants felt the patient had stage 1 hypertension.
Though most consultants agreed stage 1 hypertension does not require immediate medication, they were critical of the physician’s inaction (not taking repeat readings, considering family history of hypertension, documenting in the medical chart discussions of hypertension counseling, conducting lab studies for lipid profiles and other tests).
Most defense consultants agreed that it was a judgment call to treat this young man for borderline hypertension, and the lack of hypertension treatment had no bearing on the sudden MI. However, they all stated that the patient should have been more closely monitored with regular blood pressure checks, diagnostic labs, and counseled on modifying diet and lifestyle.
Making this case more difficult to defend was the physician’s admission at deposition that he was not clear on the standard of care in treating hypertension.
Disposition
This case was settled on behalf of the internal medicine physician.
Risk management considerations
Incomplete documentation often hinders the defense of lawsuits. Each patient encounter should include the chief complaint, examination findings and prior diagnostic tests results (if applicable), assessment, clinical impression or diagnosis, and the plan of care. Not only did this physician not support his clinical impression of the patient’s blood pressure, the only acknowledgement of the blood pressure readings was a circle around the numbers.
Completed histories are the basis for patient information. It is not unusual to have a patient complete a questionnaire before the appointment as this helps expedite the patient visit; however, reviewing the form and completing areas left blank may provide additional insight. By initialing and dating each page, a physician can provide verification that the information was reviewed.
Some consultants believed that, given the patient’s family history of hypertension, medications should have been started immediately. Most consultants agreed that education on dietary and lifestyle changes was more important the first year. Unfortunately, the patient’s chart supported the plaintiffs’ view that the physician failed to advise the patient of his cardiovascular and hypertension risk factors.
Physicians can make themselves more defensible by obtaining a complete history, documenting each patient encounter, and documenting any education provided to the patient. This assists both the patient in making informed choices and the physician, should the patient allege failure to diagnose and treat.
Google is so powerful that it “hides” other search systems from us. We just don’t know the existence of most of them.
Meanwhile, there are still a huge number of excellent searchers in the world who specialize in books, science, other smart information.
Keep a list of sites you never heard of.
http://www.refseek.com – Academic Resource Search. More than a billion sources: encyclopedia, monographies, magazines.
http://www.worldcat.org – a search for the contents of 20 thousand worldwide libraries. Find out where lies the nearest rare book you need.
https://link.springer.com – access to more than 10 million scientific documents: books, articles, research protocols.
http://www.bioline.org.br is a library of scientific bioscience journals published in developing countries.
http://repec.org – volunteers from 102 countries have collected almost 4 million publications on economics and related science.
http://www.science.gov is an American state search engine on 2200+ scientific sites. More than 200 million articles are indexed.
http://www.base-search.net is one of the most powerful researches on academic studies texts. More than 100 million scientific documents, 70% of them are free.
Using Contrast To Cut The Gordian Knot! A Complicated CTO Intervention
By Dr. Salman Arain
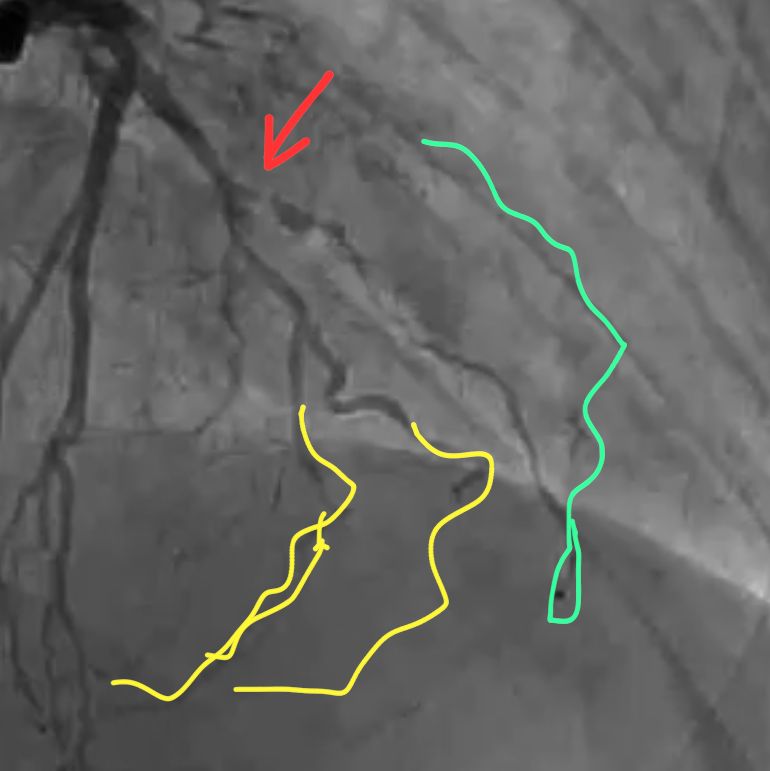
This is the complete angio. The patient is 57 years old with CCS 3 angina. He had bypass surgery 13 years ago. His EF is 35 to 40%.
Viability Study
So, the question for our Cardio experts:
1) What do you recommend? PCI, re-do CABG, EECP or OMT alone? 2) If you choose PCI, which vessel would you go after first? 3) And what CTO strategy would you use? Retrograde PCI may or may not be the best answer here. 4) What do you know about the coronary sinus reducer, and would you consider that?
Tricky. The problem with the LCX is that the caps are all ambiguous and there are several bifurcations.
The LAD CTO is long but at least there is a well defined cap and a relatively straight course. Unfortunately the LAD septals supply the PDA which itself is occluded proximally and does not connect to the PLBs.
The RCA is the trickiest of all three. One thing to keep in mind is that the patient is post CABG – so any perforations would be more difficult to treat.
Ok, here is how it all played out. First a few thoughts about choosing the vessel to intervene upon.
The LAD has the most favorable anatomy but needs to be fixed least urgently. The proximal 1/3 is patent and the mid segment has a graft.
The LCX has an ambiguous cap and several branches that need to be rescued. It is important not only because of its own distribution, but because it is the best retrograde conduit to the RCA via the PLB.
RCA is the trickiest because it requires a combined antegrade and retrograde approach. Also, the PDA is occluded and is cut off from the large PLB system. So an occluded bifurcation somewhere!
Thus, we decided to go after the LCX – it was the one that would give us the greatest advantage in addressing the RCA.
Here are some dual injection angios to better show you the connections.
There are several ways to tackle a CTO – some antegrade and some retrograde. We have focused on and specialized in contrast modulation of plaque. This requires puncturing the proximal cap and then using micro injections of contrast. The technique is also called a modified Carlino injection after Mauro Carlino who described
Here is the setup for the LCX intervention by means of CAP (aka Carlino). Notice the ambiguous cap.
This is not the typical cloud. It is tubular which means we must be extra plaque
So we used a Gaia 2 to redirect our MC and repeat the contrast injection. Now we see the vessel architecture – as well as re-entry!
This is just the injection clip. The typical result is seen towards the LCX. There contrast mediated STAR into the OM2!
So we wired the LCX first, then treated the bifurcation, and used a dual lumen catheter to wire the OM2.
We used IVUS to confirm that we were not going to jail off the side branch with our stent. We used JSBT!
And here is the final angio. You can see that we are nicely set up for a retrograde intervention on the RCA in a few weeks.
And now you have the complete name for the case: Using Contrast To Cut The Gordian Knot! A Complicated CTO Intervention
Afterword. I think this case highlights how far coronary PCI has come – as a specialty. In my fellowship, this talk of dissecting and injecting contrast and going epicardial would have been blasphemous. And now it is routine in selected centers of course.
The upshot is that CABG is no longer the end of the road. The end of the road is the end of the road – and that is not in sight for coronary PCI!!!
Dr. Zaka Khan wrote: Regarding Coronary sinus reducer – This was original developed by Neovasc . A Canadian startup. There main two products for Cosira and Tiara. Cosira was designed for controlled occlusion of CS to improve symptoms of refractory Angina . It does improve at least 1 CCS class. Would work only in cases of refractory angina and evidence of reversible ischemia. It increases coronary microvasculature flow. Tiara was supposed to be Transseptal Mitral valve replacement system without need for apical approach. Company got into litigation with Edward’s and then few guys at UPEN. Material used for Tiara was manufactured by Boston Sci and hence they jumped into the mix. Cosira system was bought into by Shockwave medical. Tiara is still somewhere and the fight goes on. Many investors lost money because of legal battles. Would have been a big hit like TAVR .
Questions by Dr. Afaq Motiwala answered by Dr. Arain:
) Does the micro catheter injection into the cap create more extensive dissection (if you are extra plaque) and make it harder to get into true lumen? Yes and no. That is where we have honed our technique. It’s all a matter of understanding the contrast cloud.
2) How did the ivus help you with side branch? It helped confirm that I was in true lumen and that the side branch was not jailed behind plaque.
3) Where did you place your balloon for jsbt? Balloon from OM2 to top branch and stent in the main body of the OM2
4)The small branch you preserved with a wire, does it have some contained hematoma? Any need to tamponade it or it’s inconsequential? It does, but the flow was good without a dissection in multiple views. So OK to follow clinically. These are very small branches.
.
It was important to preserve the OM2 trifurcation. You can see the size of it in the cranial view. The top branch fills OM1 and the bottom two supply the PLB. I plan to fix both eventually.
Dr. Amin H. Karim wrote: The cath diagram took me back to pre-EMR days when we routinely made these after watching the cine on Trajano. They were very reflective of the coronary anatomy as well as recording one’s personal notes. 30 years later when we look at these in the patient’s chart it gives a good idea of the pre-intervention anatomy. Computer diagrams are no match and I feel sorry for your younger colleagues when they pull their patient records decades later, they will be looking at a computer cartoon that is a far cry from the real anatomy. Both Michael DeBakey and Denton Cooley gave a lot of importance to the cath diagram on patients referred for surgery and both would hang them on the old x-ray box in the OR as a reference! Dr. DeBakey would meticulously put his pencil notes on the diagram and file them on each patient. He would also draw the grafts on another copy and send them to the referral cardiologist. He would pull the file out when patient came in years later for redo
Here is a way to think (and talk) about left main PCI.
A – Anatomy (i.e. functional anatomy) which includes angiography, IVUS, and physiology. B – Bifurcation classification If applicable of course. C – Calcium management. All inclusive term that includes all available devices for lesion preparation: rota, CSI, IVL, cutting balloons, laser, and of course NC balloons. D – Devices. This includes the need for and choice of mechanical support. E – Execution. The actual PCI strategy (or strategies).
86 year old man with patent LIMA and SVG to RCA. Now with exertional angina and lateral wall ischemia (large).
Here is the LIMA shot from then – the proximal segment of the LAD is not supplied by the graft. So worth saving and/or protecting.
Here are my ABCDEs – as promised.
A: Functionally and anatomically the calcium involves all three branches. FFR or iFR not needed.
B: This is a Medina 1,1,1. The proximal LAD supplies a significant area and is worth saving.
C: There is nodular calcium and some type of atherectomy will help place stents. My first choice was rotational atherectomy given that it is a front cutter.
D: This is a protected LM and the EF is low normal. So no need for an MCS.
E: The LM is very short or non-existent. This anatomy is better suited for Culotte though any technique would work.
S: Not applicable.
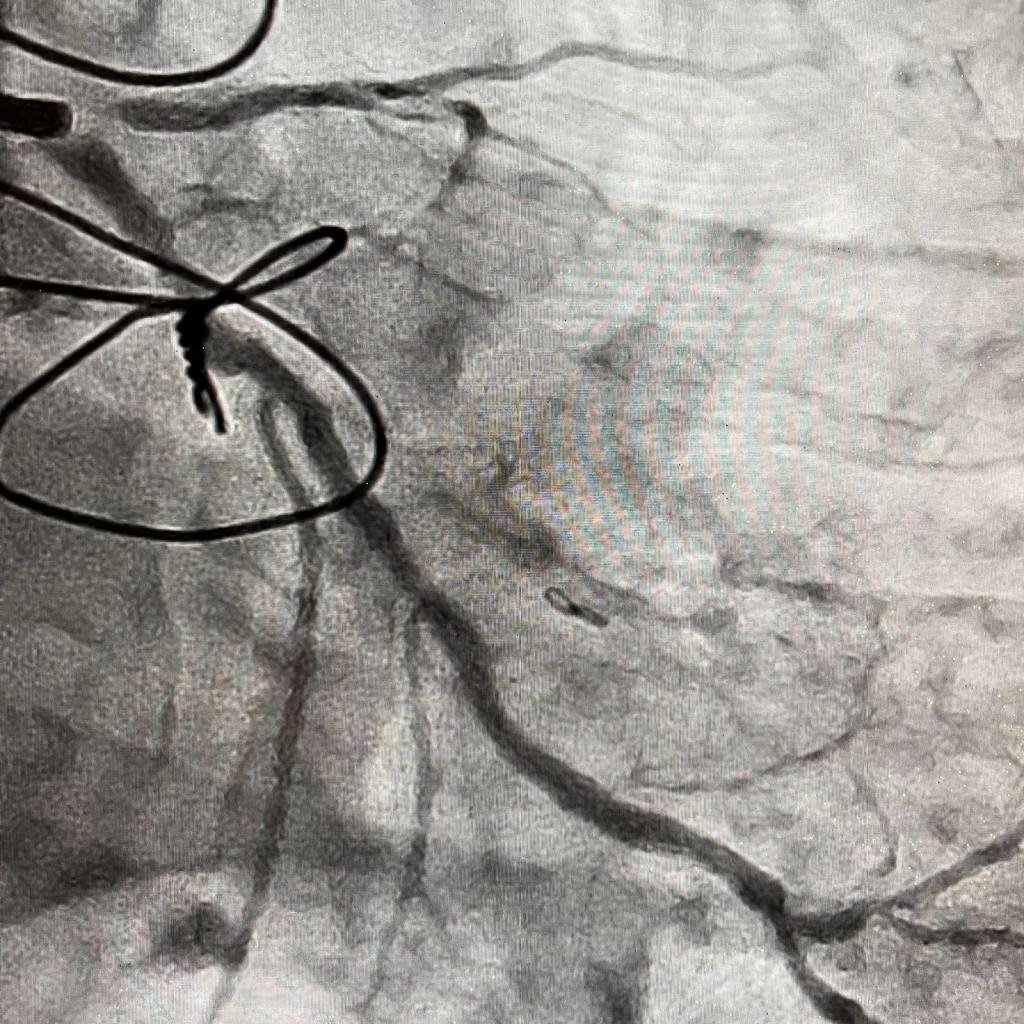
We ended up wiring the LM into the LCX followed by atherectomy with a 1.5 burr. We were unable to wire the proximal LAD from the LM because the ostium was obstructed by the calcium nodule.
And here is the final result.
You can see that the LCX is technically a first OM that supplies a major portion of the lateral wall with its 5(!) branches.