
This a recording of the CME Talk at the Shahabuddin Rahmtulla Symposium prsented by the Association of American-Descent Cardiologists of North America (APCNA) at the 49th Annual Convention of Association of Pakistan–Descent Physicians of North America (APPNA) on July 4 2026 in Orlando, Florida. USA.
Table of Contents
Lipoproten (a) Management
Lipfendra and the Emerging Era of Lipoprotein(a) Management:
A Clinical Review
Authors:

Noe Rodrigo Martínez-Paredes, Medical Intern (Hospital de los Maestros SNTE Sección 50, Monterrey, Mexico).
- Amin H. Karim, MD, Baylor College of Medicine, Houston, Texas and Institute for Academic Medicine, Houston, Texas.
ABSTRACT
Elevated Lipoprotein(a) [Lp(a)] is an independent, genetically driven, and highly prevalent risk factor for atherosclerotic cardiovascular disease (ASCVD) and calcific aortic valve stenosis (CAVS). While traditional statin therapies effectively lower low-density lipoprotein cholesterol (LDL-C) via hepatic receptor upregulation, they consistently fail to reduce Lp(a) levels and may paradoxically increase them. This review highlights the critical transition toward precision cardiovascular pharmacology, focusing on Lipfendra (enlicitide)—a breakthrough oral PCSK9 inhibitor—and the revolutionary development of RNA-targeted therapies designed to definitively silence hepatic Lp(a) production.
1. THE LIPOPROTEIN(a) CHALLENGE
Lp(a) is recognized as one of the most atherogenic and pro-thrombotic lipoproteins in human plasma, yet it remains significantly underdiagnosed in standard clinical practice.
- Genetic Determinism: Unlike LDL-C, which is heavily influenced by diet, exercise, and metabolic syndrome, circulating Lp(a) levels are up to 90% genetically determined by the LPA gene locus on chromosome 6. Lifestyle modifications have virtually zero impact on its concentration.
- Unique Pathophysiology: Lp(a) consists of a standard LDL-like particle covalently bound to a highly specific glycoprotein called apolipoprotein(a) [apo(a)].
- Pro-Thrombotic Nature: The molecular structure of apo(a) is highly homologous to plasminogen. This structural mimicry allows Lp(a) to competitively inhibit plasminogen activation on the surface of fibrin clots, thereby impairing natural fibrinolysis and promoting a pro-thrombotic state.
- Vascular Inflammation and Stenosis: Lp(a) serves as the primary carrier of oxidized phospholipids (OxPL) in the bloodstream. When deposited in the arterial intima, these OxPLs recruit monocytes, driving foam cell formation. In the aortic valve, they trigger an inflammatory cascade that leads to osteogenic differentiation, making Lp(a) a primary driver of CAVS.
2. THE STATIN PARADOX AND THERAPEUTIC LIMITS
Standard HMG-CoA reductase inhibitors (statins) are the undeniable foundation of ASCVD primary and secondary prevention. However, their mechanism reveals a critical vulnerability when managing elevated Lp(a).
- Mechanism Failure: Statins lower plasma cholesterol by inhibiting hepatic cholesterol synthesis, which subsequently upregulates LDL receptors (LDLR) on the hepatocyte surface. However, because the apo(a) moiety physically shields the binding domains of the Lp(a) particle, it has a extremely weak affinity for the LDLR. Consequently, statin-induced LDLR upregulation clears LDL-C but leaves Lp(a) circulating.
- Paradoxical Elevation: Extensive clinical registry data and meta-analyses have demonstrated that statin therapy can actually increase Lp(a) serum levels by 10% to 20%. This is believed to occur due to a compensatory intracellular mechanism where the depletion of hepatic cholesterol triggers an increase in the transcription of both PCSK9 and the LPA gene.
- The Residual Risk: Patients on high-intensity statins who achieve optimal LDL-C targets but have persistent Lp(a) elevations remain at a profoundly high risk for recurrent myocardial infarctions and ischemic strokes.
3. EMERGING THERAPIES: TARGETED MECHANISMS OF ACTION
To address this residual atherothrombotic risk, novel pharmacological pathways bypass the standard HMG-CoA reductase mechanisms entirely.
A. Oral PCSK9 Inhibition (Lipfendra / Enlicitide)
- The Pharmacological Barrier: Historically, PCSK9 inhibitors required subcutaneous injections because peptides are rapidly degraded by gastrointestinal enzymes and possess poor epithelial permeability. Lipfendra utilizes a specialized macrocyclic peptide structure designed to overcome the gastric environment and achieve efficient systemic absorption.
- Mechanism of Action: Once absorbed into the portal circulation, Lipfendra binds with exceptionally high affinity to circulating PCSK9 protein. By neutralizing PCSK9, it prevents the lysosomal degradation of LDLRs, dramatically extending their lifecycle on the hepatocyte surface.
- Clinical Efficacy: It is the first once-daily oral PCSK9 inhibitor, dramatically improving patient adherence. While its primary role is achieving massive LDL-C reductions (up to 50%), it also provides a modest, yet clinically relevant, secondary reduction in Lp(a) of approximately 20% to 30%.
- Advantages Over Injectables and Traditional Therapies: While monoclonal antibodies targeting PCSK9 (evolocumab, alirocumab) offer profound LDL-C reduction, they present significant logistical and psychological barriers, including the need for subcutaneous administration, cold-chain storage, injection-site reactions, and reduced long-term adherence due to needle fatigue. Lipfendra bridges this gap by delivering “biologic-level” efficacy in a convenient oral formulation. Furthermore, it overcomes the limitations of other traditional lipid-lowering classes. Unlike statins, which can paradoxically raise Lp(a) and cause debilitating myalgias, or ezetimibe and bempedoic acid, which provide only modest LDL-C reductions (15% to 25%), Lipfendra offers aggressive LDL-C lowering paired with a targeted reduction in Lp(a) without inducing muscle toxicity.
- Safety Profile and Adverse Effects: Data from clinical trials indicate that enlicitide is highly tolerable. Because its mechanism of action is entirely extracellular and does not interfere with intracellular cholesterol synthesis like statins, it effectively eliminates the risk of statin-associated muscle symptoms (SAMS). The most commonly reported adverse effects are mild, transient, and primarily gastrointestinal—such as nausea, flatulence, or mild dyspepsia—which are often associated with the strict fasting conditions required for optimal absorption. Clinically significant hepatotoxicity or severe systemic immunogenic reactions have not been observed, making it an exceptionally favorable option for statin-intolerant patients.
B. RNA-Based Genetic Silencing (ASOs and siRNAs)
These therapies represent the ultimate precision medicine approach, targeting the LPA mRNA directly in the hepatocyte to prevent the translation of the apo(a) protein. Without apo(a), the complete Lp(a) particle cannot be assembled.
- Antisense Oligonucleotides (Pelacarsen): This ASO binds specifically to the transcribed LPA mRNA. Upon binding, it recruits RNase H1, an intracellular enzyme that degrades the target RNA strand. Administered via monthly subcutaneous injection, it achieves an ~80% reduction in circulating Lp(a).
- Small Interfering RNAs (Olpasiran / Lepodisiran): Conjugated with GalNAc to specifically target hepatocyte receptors, siRNAs utilize the natural RNA-induced silencing complex (RISC) to continuously cleave LPA mRNA. Because the RISC complex is highly catalytic, a single subcutaneous injection can provide a sustained >95% reduction in Lp(a) for 3 to 6 months.
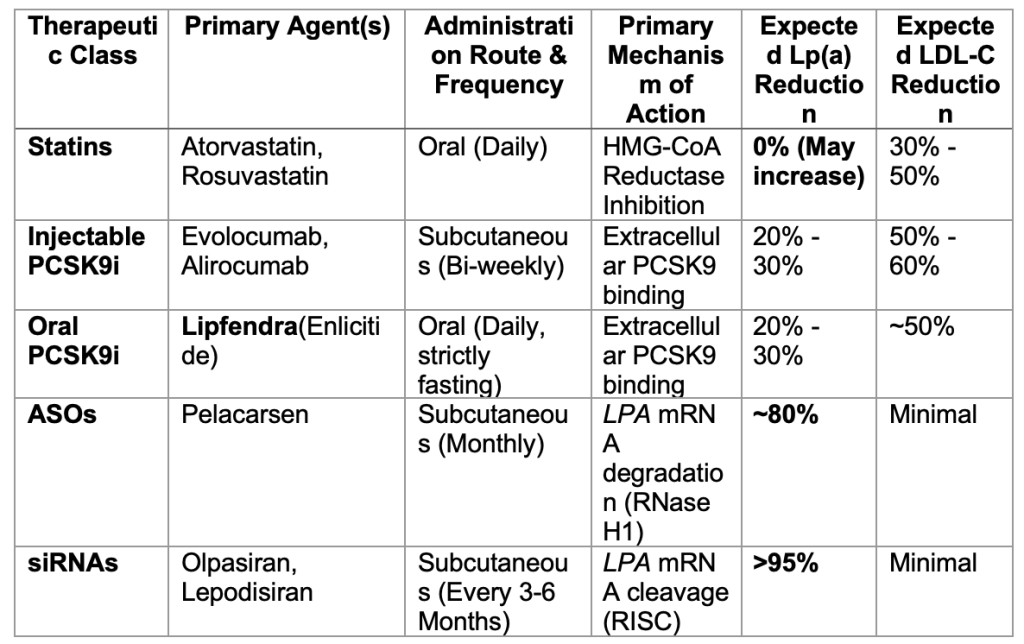
4. COMPARISON OF ADVANCED LIPID-LOWERING MODALITIES
The landscape of lipid management is rapidly evolving beyond standard statin therapy. Selecting the appropriate pharmacological agent now requires a nuanced understanding of a patient’s specific lipid profile, particularly when addressing residual risks associated with isolated Lp(a) elevations versus primary LDL-C management. The following table provides a comprehensive overview of the primary mechanisms, administration routes, and expected efficacies of both established and emerging lipid-lowering therapies, highlighting the distinct advantages of oral PCSK9 inhibitors and RNA-targeted silencing.
5. CLINICAL PRACTICE & FUTURE GUIDELINES
- Universal Screening: Recognizing the hidden danger of genetic dyslipidemias, major cardiovascular societies (including the ACC/AHA and the ESC) now strongly recommend measuring Lp(a) at least once in an adult’s lifetime to identify individuals with inherited ASCVD risk.
- Dosage and Administration of Lipfendra: Based on advanced clinical trials, the optimal therapeutic dosage for enlicitide ranges from 20 mg to 30 mg taken once daily. For optimal bioavailability, this once-daily dose must be administered on a strictly empty stomach, at least 30 minutes before the first meal or beverage of the day. This strict fasting is crucial, as the gastrointestinal absorption of these oral peptides is drastically reduced in the presence of food and active gastric secretions. Routine monitoring of liver function is standard practice, although hepatotoxicity rates remain minimal.
- The Horizon of Cardiology: If ongoing Phase 3 cardiovascular outcomes trials (such as the HORIZON trial for Pelacarsen) demonstrate a definitive reduction in Major Adverse Cardiovascular Events (MACE), RNA-targeted therapies will swiftly transition to Class I guideline recommendations, establishing a new gold standard for isolated Lp(a) elevation.
6. KEY CLINICAL TAKEAWAYS
- Lp(a) is statin-resistant and genetically driven: Routine lipid panels and standard statin prescriptions are fundamentally insufficient for patients harboring genetic Lp(a) elevations.
- Lipfendra changes patient compliance: As a breakthrough oral PCSK9 inhibitor, it offers powerful LDLR upregulation without the psychological and physical burden of long-term injectable therapies.
- RNA therapies are the definitive solution: By intercepting and silencing the LPA gene directly in the liver, ASOs and siRNAs can nearly eradicate circulating Lp(a), promising to close the gap on residual cardiovascular risk.
REFERENCES
- Reyes-Soffer G, Ginsberg HN, Berglund L, et al. Lipoprotein(a): A Genetically Determined, Causal, and Prevalent Risk Factor for Atherosclerotic Cardiovascular Disease: A Scientific Statement From the American Heart Association. Arterioscler Thromb Vasc Biol. 2022;42(1):e48-e60.
- Tsimikas S. A Test in Context: Lipoprotein(a): Diagnosis, Prognosis, Controversies, and Emerging Therapies. J Am Coll Cardiol. 2017;69(6):692-711.
- Kronenberg F, Mora S, Stroes ESG, et al. Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: a European Atherosclerosis Society consensus statement. Eur Heart J. 2022;43(39):3925-3946.
- Zheng KH, Tsimikas S, Pawade T, et al. Lipoprotein(a) and Oxidized Phospholipids Promote Valve Calcification in Patients With Aortic Stenosis. J Am Coll Cardiol. 2019;73(17):2150-2162.
- Tsimikas S, Gordts PLSM, Nora C, Yeang C, Witztum JL. Statin therapy increases lipoprotein(a) levels. Eur Heart J. 2020;41(24):2275-2284.
- Willeit P, Ridker PM, Nestel PJ, et al. Baseline and on-statin treatment lipoprotein(a) levels for prediction of cardiovascular events: individual patient-data meta-analysis of statin outcome trials. Lancet. 2018;392(10155):1311-1320.
- Nissen SE, Wolski K, Prcela L, et al. Efficacy and Safety of an Oral PCSK9 Inhibitor in Statin-Treated Patients: A Phase 2 Randomized Clinical Trial. JAMA Cardiol. 2023;8(5):455-462.
- Ballantyne CM, Banka P, Mendez G, et al. Phase 2b Randomized Trial of the Oral PCSK9 Inhibitor MK-0616. J Am Coll Cardiol. 2023;81(16):1553-1564.
- Nurmohamed NS, Dullaart RPF, Stroes ESG. Oral PCSK9 inhibitors: A new era of accessible lipid-lowering therapy? Curr Opin Lipidol. 2024;35(1):15-21.
- O’Donoghue ML, Rosenson RS, Gencer B, et al. Small Interfering RNA to Reduce Lipoprotein(a) in Cardiovascular Disease (Olpasiran). N Engl J Med. 2022;387(20):1855-1864.
- Tsimikas S, Karwatowska-Prokopczuk E, Gouni-Berthold I, et al. Lipoprotein(a) Reduction in Persons with Cardiovascular Disease (Pelacarsen). N Engl J Med. 2020;382(3):244-255.
- Nissen SE, Wolski K, Balog C, et al. Single Ascending Dose Study of a Short Interfering RNA Targeting Lipoprotein(a) Production in Individuals With Elevated Plasma Lipoprotein(a) Levels (Lepodisiran). JAMA. 2023;330(21):2075-2083.
- Katzmann JL, Laufs U. Pharmacological lowering of Lipoprotein(a). Curr Opin Lipidol. 2023;34(3):133-140.
- Grundy SM, Stone NJ, Bailey AL, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol. Circulation. 2019;139(25):e1082-e1143.
- Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111-188.
Apixaban and Anticoagulation Correlation
Asli Hacioglu MD
Gazi University, Ankara, Turkey

and
Hareesha Rishab MBBS, National Health Service, United Kingdom
Amin H. Karim MD, Baylor College of Medicine, Houston, Texas and Institute for Academic Medicine, Houston, Texas
Artificial Intelligence in Cardiology
By
Ajala GLoria Eyitayo
All Saints University School of Medicine
Diego Gomez de la Garza
Universidad de Monterrey, Mexico
Amin H. Karim MD
Baylor College of Medicine
Houston, Texas
Recent Clinical Observer Group 2026
Students are given opportunity to study a case and write up a talk for the other students:




Students from Nigeria, Pakistan, Mexico, India, Nepal. 2026.

Observers from Turkey, Mexico, USA, Indonesia. April 2026

Observers and medical students from Pakistan, Nigeria Mexico, Peru, Turkey.

Observers watching grand rounds.
Peri-operative Cardiovascular Medication Management for Non-cardiac Surgery.

By Jessica Eve (Java, Indonesia)
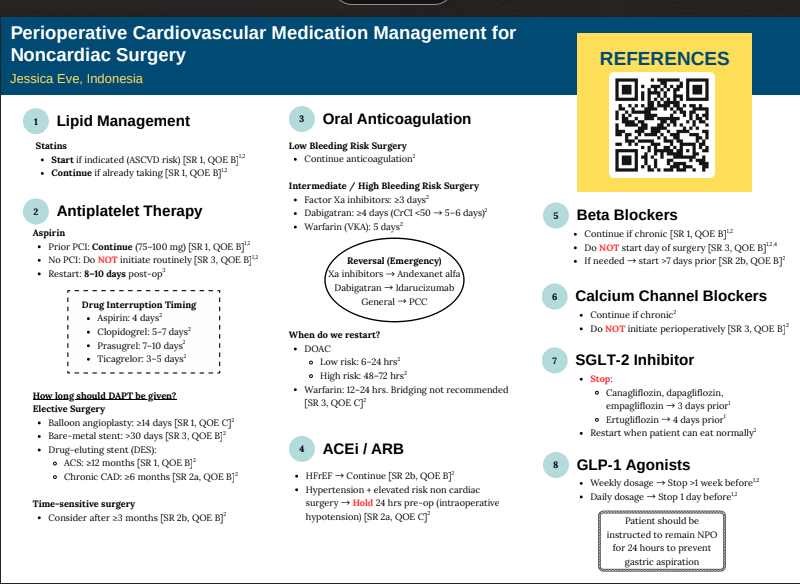
REFERENCES
- Winchester DE, Mehta JJ, Alexander JT. Perioperative cardiovascular medication
management for noncardiac surgery. JAMA. Published online March 31, 2026.
doi:10.1001/jama.2026.0067 - American Heart Association. 2024 AHA/ACC guideline for perioperative cardiovascular
evaluation and management of patients undergoing noncardiac surgery. Circulation.
2024;150:e351–e442. doi:10.1161/CIR.0000000000001285 - Devereaux PJ, Mrkobrada M, Sessler DI, Leslie K, Alonso-Coello P, Kurz A, et al;
POISE-2 Investigators. Aspirin in patients undergoing noncardiac surgery. N Engl J Med.
2014;370(16):1494–1503. doi:10.1056/NEJMoa1401105 - Devereaux PJ, Yang H, Yusuf S, Guyatt G, Leslie K, Villar JC, et al; POISE Study
Group. Effects of extended-release metoprolol succinate in patients undergoing non-
cardiac surgery (POISE trial): a randomised controlled trial. Lancet.
2008;371(9627):1839–1847. doi:10.1016/S0140-6736(08)60601-7 - Neumann A, Maura G, Weill A, Alla F, Danchin N. Clinical events after discontinuation of
β-blockers in patients without heart failure optimally treated after acute myocardial
infarction: a cohort study on the French healthcare databases. Circ Cardiovasc Qual
Outcomes. 2018;11(4):e004356. doi:10.1161/CIRCOUTCOMES.117.004356 - Lindenauer PK, Pekow P, Wang K, et al. Lipid-lowering therapy and in-hospital
mortality following major noncardiac surgery. JAMA. 2004;291(17):2092-2099.
doi:10.1001/jama.291.17.2092 - London MJ, Schwartz GG, Hur K, Henderson WG. Association of perioperative
statin use with mortality and morbidity after major noncardiac surgery. JAMA Intern
Med. 2017;177(2):231-242. doi:10.1001/jamainternmed.2016.8005 - Berwanger O, de Barros E Silva PG, Barbosa RR, et al. Atorvastatin for high-
risk statin-naïve patients undergoing noncardiac surgery. Am Heart J. 2017;184:88- - doi:10.1016/j.ahj.2016.11.001
- Graham MM, Sessler DI, Parlow JL, et al. Aspirin in patients with previous
percutaneous coronary intervention undergoing noncardiac surgery. Ann Intern Med.
2018;168(4):237-244. doi:10.7326/M17-2341 - Kobori T, Onishi Y, Yoshida Y, et al. Association of glucagon-like peptide-1
receptor agonist treatment with gastric residue in an esophagogastroduodenoscopy.
J Diabetes Investig. 2023;14(6):767-773. doi:10.1111/jdi.14005 - Joshi GP, LaMasters T, Kindel TL. Preprocedure care of patients on glucagon-
like peptide-1 receptor agonists. Anesthesiology. 2024;141(6):1208-1209.
doi:10.1097/ALN.0000000000005231
Heart Failure With Preserved Ejection Fraction and Atrial Fibrillation: Egg or the Chicken
Heart Failure with Preserved Ejection Fraction and Atrial
Fibrillation: What was first, the Egg or the Chicken?
Laiba Ejaz
Karachi Institute of Medical Sciences.
Samuel Sotelo Hernandez
Autonomous University of Durango-Cappus Zacatecas
Amin H. Karim MD
Methodist Academy of Medicine, Houston, Texas
Abstract
A 68-year-old African American man presented with recurrent lower extremity edema without dyspnea or chest pain. His history included hypertension, hyperlipidemia, and obesity. Evaluation revealed atrial fibrillation with a
controlled ventricular rate and echocardiographic findings consistent with heart failure with preserved ejection fraction (HFpEF). Secondary causes such as deep venous thrombosis were excluded. The patient was managed
with metoprolol and diuretics for rate and volume control, losartan and hydrochlorothiazide for hypertension, apixaban for anticoagulation, and amiodarone for rhythm stabilisation. After a year of persistent atrial
fibrillation, elective cardioversion successfully restored sinus rhythm following confirmation of the absence of atrial thrombus on transesophageal echocardiography. The patient remained clinically stable on subsequent
follow-up visits.
Introduction
Atrial fibrillation (AF) and heart failure with preserved ejection fraction (HFpEF) are common cardiovascular conditions that frequently coexist, particularly in older, hypertensive, and obese patients. AF can exacerbate
HFpEF by impairing atrial contribution to ventricular filling, while HFpEF may predispose to atrial remodelling and subsequent arrhythmia, creating a complex bidirectional relationship. Both conditions independently
increase morbidity and mortality and pose challenges in diagnosis and management, especially when symptoms such as edema or fatigue are subtle or overlapping. Understanding the temporal relationship between AF and
HFpEF is critical for optimizing therapy, including rate versus rhythm control, anticoagulation, and management of comorbidities. This case highlights a patient with recurrent lower extremity edema, AF, and HFpEF, raising
the clinical question of which condition preceded the other and illustrating the importance of individualized, comprehensive cardiovascular care.
Case Presentation
A 68-year-old African American man presented to the clinic with complaints of recurrent fluid buildup, mainly in his lower extremities, as noted by his primary care physician. He denied dyspnea, chest pain, orthopnea, or
paroxysmal nocturnal dyspnea. His medical history included hypertension, hyperlipidemia, and obesity. He reported occasional alcohol use and denied smoking. His family history was significant for coronary artery
disease, hypertension, hyperlipidemia, and diabetes mellitus. On examination, his weight was 280 lbs (127 kg) and height 73 inches, yielding a BMI of 37.7 kg/m2, consistent with Class I obesity. Blood pressure ranged
between 135–145/75–85 mmHg, and his pulse was irregular at 58–70 beats per minute.
Laboratory
investigations revealed a normal HbA1c and a lipid profile with total cholesterol 222 mg/dL, HDL 67 mg/dL, LDL 149 mg/dL, and triglycerides 60 mg/dL. An electrocardiogram (EKG) (figure 1) obtained during the initial
visit showed atrial fibrillation with a controlled ventricular rate of approximately 58 beats per minute. A subsequent 2D echocardiogram demonstrated a preserved left ventricular ejection fraction of 60–65% and mild
left atrial enlargement—findings consistent with heart failure with preserved ejection fraction (HFpEF). Chest X-ray showed chronic airway changes and mild atherosclerosis, while Doppler ultrasound ruled out deep
venous thrombosis. The patient was started on metoprolol and diuretics for rate and volume control, along with losartan and hydrochlorothiazide for blood pressure management. Anticoagulation with Eliquis (apixaban) and
rhythm control with amiodarone was initiated and continued for over a year without spontaneous conversion to sinus rhythm (figure 2). He subsequently underwent elective cardioversion, which successfully restored sinus
rhythm (figure 3) A transesophageal echocardiogram prior to the procedure confirmed the absence of thrombus in the left atrium or left atrial appendage. The patient continued regular follow-up and remained clinically stable
thereafter.
Discussion
This case highlights the complex interplay between atrial fibrillation (AF), hypertension, obesity, and heart failure with preserved ejection fraction (HFpEF) in an older African American male. The patient’s presentation
with peripheral edema, in the absence of dyspnea or orthopnea, emphasises that HFpEF can manifest subtly and that careful evaluation of cardiovascular risk factors and cardiac rhythm is essential for accurate diagnosis and
management (1,2). Atrial fibrillation is a common arrhythmia in elderly individuals, often associated with structural heart changes such as left atrial enlargement and diastolic dysfunction. In this patient, chronic
hypertension and obesity likely contributed to increased left ventricular stiffness and impaired relaxation, leading to diastolic dysfunction and, consequently, HFpEF (3,4). The echocardiographic findings of preserved left
ventricular ejection fraction (60–65%) with mild left atrial enlargement are consistent with this diagnosis. The irregularly irregular rhythm on electrocardiogram confirmed the presence of AF, while the controlled ventricular rate suggested adequate rate control with beta-blocker therapy (5).
HFpEF accounts for nearly half of all heart failure cases, and its prevalence continues to rise in parallel with obesity, hypertension, and metabolic syndrome (1,6). Pathophysiologically , the combination of increased
ventricular wall stress, endothelial dysfunction, and myocardial fibrosis results in elevated filling pressures despite normal systolic function (7). This leads to symptoms such as lower extremity edema, exercise intolerance, or mild dyspnea, which may fluctuate depending on volume status. Importantly, obesity is a key modifiable factor that exacerbates both HFpEF and AF by promoting systemic inflammation, left atrial remodelling, and neurohormonal activation (6,7). The management of this patient was appropriately focused on
controlling heart rate, optimizing blood pressure, managing volume status, and preventing thromboembolic events. Beta-blocker therapy (metoprolol) was effective for rate control, while diuretics addressed the peripheral
edema. Losartan and hydrochlorothiazide provided additional blood pressure control and diuresis. Given the patient’s CHA2DS2-VASc score—elevated due to age, hypertension, and heart failure—anticoagulation with
apixaban was warranted to reduce the risk of stroke, which is fivefold higher in individuals with AF (5,8). Despite more than a year of rate control and anticoagulation, the patient did not experience spontaneous
reversion to sinus rhythm. Therefore, elective cardioversion was pursued, preceded by transesophageal echocardiography to rule out intracardiac thrombus. The successful restoration of sinus rhythm improved cardiac
efficiency and potentially reduced the risk of HF progression (9). Ongoing rhythm surveillance is essential, as recurrence of AF is common, particularly in patients with underlying structural heart disease and obesity (10).
From a preventive perspective, aggressive risk factor modification remains a cornerstone of long -term management. Weight reduction, dietary sodium restriction, and increased physical activity can improve diastolic
function and reduce AF recurrence (1,2). Additionally, lipid lowering with statin therapy is indicated given the elevated LDL cholesterol level (149 mg/dL), further reducing cardiovascular risk (3,6).
In summary, this case underscores the importance of a multidisciplinary approach in managing AF and HFpEF , particularly in patients with multiple cardiovascular risk factors. Optimal control of hypertension, obesity, and
dyslipidemia, combined with rhythm management and anticoagulation, can lead to favorable clinical outcomes. The patient’s successful cardioversion and stable follow-up course demonstrate that with comprehensive care,
symptom control and maintenance of sinus rhythm are achievable in this complex patient population.
References:
- Kittleson MM, Panjrath GS, Amancherla K, et al. 2023 ACC Expert Consensus Decision
Pathway on Management of Heart Failure With Preserved Ejection Fraction. J Am Coll Cardiol.
2023;81(18):1835–78. doi:10.1016/j.jacc.2023.03.393 - American College of Cardiology. 2024 ACC Expert Consensus Decision Pathway on
Clinical Assessment, Management, and Trajectory of Patients Hospitalized With Heart Failure. J Am Coll
Cardiol. 2024. doi:10.1016/j.jacc.2024.06.002 - American College of Cardiology/American Heart Association. 2024 Update to the 2020
ACC/AHA Clinical Performance and Quality Measures for Adults With Heart Failure. Circ Heart Fail/HCQ. - doi:10.1161/HCQ.0000000000000132
- Riccardi M, et al. Current Treatment of Heart Failure with Preserved Ejection Fraction. J
Clin Med. 2025;14(15):5406. doi:10.3390/jcm14155406 - European Society of Cardiology. 2024 ESC Guidelines for the Management of Atrial
Fibrillation. Eur Heart J. 2024. Available from:
https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Atrial-Fibrillation - Shahid M, et al. A Contemporary Review on Heart Failure with Preserved Ejection
Fraction. Front Cardiovasc Med. 2024. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12060923/ - Romanò M, et al. Heart Failure Syndromes: Different Definitions of Ejection Fraction and
Implications. J Clin Med. 2025;14(14):5090. doi:10.3390/jcm14145090 - Spotlight on the 2024 ESC/EACTS Management of Atrial Fibrillation. Eur Heart J
Cardiovasc Pharmacother. 2025. doi:10.1093/ehjcvp/pvad014 - Drug Therapy for Acute and Chronic Heart Failure with Preserved Ejection Fraction.
PubMed Central (PMC). 2025. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11093799/ - Hoevelmann J. What’s New in Heart Failure? PubMed Central (PMC). 2025 Sep. Available
from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12502451/
Clinical Student’s Companion
In 1977 I wrote up a small booklet called CLINICAL STUDENTS COMPANION and had it published by AzamSons, a book seller across from Dow Medical College. It was basically notes on General Medicine I made for the Final Professional MBBS Exam. It was common for oral examiners to ask for causes of symptoms, signs or abnormal lab values. This helped junior students to brush up on lists of causes which one could not find easily from text books of Medicine like Davidson or Harrison or Cecil Loeb. I then published two more editions wht last one being what is being uploaded here, a 260 page book with illustrations. The third edition was typed by me on the old manual Smith Corona portable type-writer.
One technique we learnt from teachers like Prof. S.M Rab (with whom I did my first intership in Medicine at Jinnah PostGraduate Medical Center, Karachi) was to think about the causes of a presentation or symptom or sign one at a time. If patient has 2-4 signs think of all the causes separately and try to figure what runs common to all the lists. This may lead one to correct diagnosis. For example when presented with Fever of Unknown Origin, think of the causes and if the patient also has anemia and splinter hemorrhages, one would find that bacterial endocarditis is present in all the 3 lists. Same for other problems.
Hope you enjoy reading. Mind you this is 45 years ago and applies to diseases found commonly in Pakistan and India. It’s value at this stage may be more historical than actual since everything now is a mouse click away on ChatGPT! 🙂 Amin H. Karim MD September 25 2025
Circ Under Duress
A CASE OF POSTOPERATIVE COMPLICATION OF SURGICAL MITRAL VALVE REPLACEMENT.
Amin H. Karim MD
CASE:
A 71 year olf Caucasian male with history of hypertension and hyperlipidemia, and chronic atrial fibrillation, developed non-rheumatic mitral valve regurgitation secondary to mitral valve prolapse, which had gradually progressed over a decade years to severe regurgitation, accompanied by moderately severe tricuspid regurgitation. Patient tolerated the valvular lesions for many years till he became symptomatic with NYHA Class III dyspnea and agreed for intervention.
CARDIAC MRI: In November 2024, cardiac MRI revealed bi-leaflet mitral valve prolapse, with severe left atrial enlargement and moderate tricuspid regurgitation. The global ejection fraction was 65% with biventricular dilatation, and basal and mid inferolateral wall scarring. Mitral and tricuspid annulus were dilated.
TWO DIMENSIONAL ECHOCARDIOGRAM: On Echocardiogram, right ventricular function was low normal. Left ventricular ejection fraction was normal. There was mitral valve prolapse due to myxomatous degeneration, severe mitral regurgitation with regurgitation fraction of 51% and estimated regurgitant volume of 56 ml. Pulmonary artery pressures were normal. Cardiac catheterization showed normal coronaries
With a low BMI and good overall health, he was felt by the cardiovascular surgeon to be low risk for surgery and MitraClip therefore not warranted.
MITRAL VALVE REPAIR SURGERY:
Mitral valve repair with a 34 mm physio 2 flexible annuloplasty ring; Intra-aortic balloon pump; Tricuspid valve repair with a 28 mm triad rigid ring; Biatrial maze utilizing the encompass clamp, RF clamp and cryoprobe; Left atrial appendage ligation with a 45 mm atrial cure mini atrial clip:
Following mitral valve repair there was no mitral regurgitation with a long segment of coaptation beneath the annular plane. The transmitral gradient was 1 mm Hg. Similarly following tricuspid valve repair there was no regurgitation with the trans tricuspid valve gradient of 1 mm.
Following bi-atrial maze procedure, the patient converted to sinus rhythm. However, when the cardio pulmonary bypass was reversed and the patient was being closed, he went to ventricular fibrillation followed by defibrillation. Frequent PVCs were observed. Intravenous amiodarone and magnesium were started; His blood pressure started to drop and vasopressors were increased and intra-aortic balloon placed. His hemodynamics improved and was watched in the OR with echo. There was inferior wall hypokinesis. He was maintained on low dose dobutamine, vasopressin and norepinephrine. His global ejection fraction was reasonable; chest was closed, but before he could be transferred out of OR he developed ventricular fibrillation again. His chest was opened and direct cardiac massage and cardioversion done with return of circulation. ECMO (Extracorporeal Membrane Oxygenation) was initiated. He was transferred to the cardiac cath lab and underwent emergency coronary angiography.
CORONARY INTERVENTION: Coronary angiography showed the dominant left circumflex was occluded in the mid potion.
IVUS showed possible edema around the left circumflex and it was felt that the circumflex was occluded due to pressure from the mitral valve ring. Stent was placed with recanalization. Impella was placed in the cath lab and the intra-aortic balloon was removed.
Intavascular Ultrasound (IVUS) shows the edema/hematoma? aeound the left vircumflex artery.
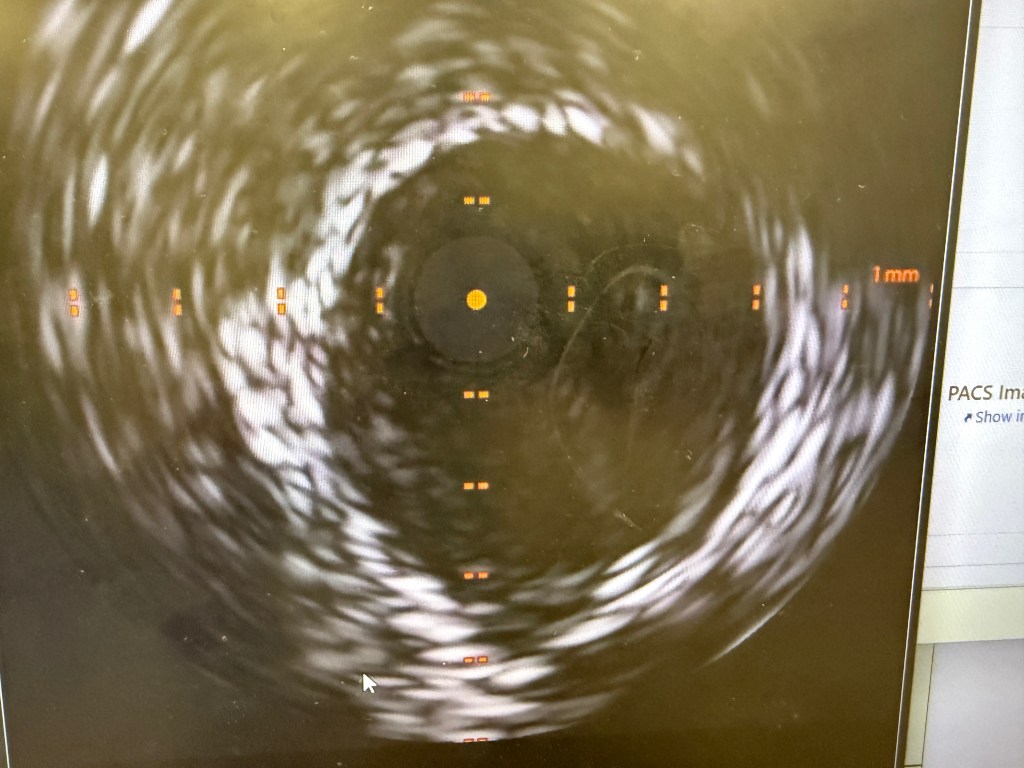
A 3.5 mm x 32 mm Synergy drug eluting stent was placed in the mid circumflex coronary artery with a good result. The intra-aortic balloon was removed.
INTENSIVE CARE UNIT: Patient remained with supported blood pressure, with severe anemia needing multiple blood transfusions. Transesophageal echo showed severely depressed right and left ventricular systolic function.
Patient was taken back to O.R. for exploration and washout. On return to ICU noted to have ST elevation in lead VII. Taken back to cath lab and coronary angiography done showing that the circumflex stent was patent.
FOLLOWUP: 10 days after mitral and tricuspid valve repair and coronary intervention, patient is off ECMO, and on Impella support. He is awake but does not follow commands. His global ejection fraction on echocardiogram is mildly depressed (40-45%) with trace of mitral and tricuspid regurgitation.
The Case of Asymptomatic Aortic Stenosis: Lessons in Patient Education and Early Symptom Recognition
Authors:
Ana Maria Sierra Valiente
Universidad Anahuac Mexico Norte
Joy Emem Efik, MBBS
Sumy State University
Ayesha Asghar, MBBS
Multan Medical and Dental College, Pakistan.
Sarai Anayansi Zárate Chavez
Universidad Anahuac Oaxaca
Amin H. Karim MD, FRCP
Baylor College of Medicine, Houston
Academy of Medicine, Houston
Weill Medical College of Cornell University.
