Authors: Tejaswini Potlabathini, Elaine Tran, PA Student, University of Texas Medical Branch, Galveston, Tx. Amin H. Karim MD FRCP FACC
Patient Overview
A 72-year-old female with a past medical history of hypertension, hyperlipidemia, hypothyroidism, and prediabetes presented to the cardiology clinic for a routine follow-up. On examination, she was found to have a firm, nodular thickening of tissue on one palm over the third metacarpal area, associated with nearby skin puckering, prompting a presumptive diagnosis of Dupuytren’s contracture.
Description
Dupuytren’s contracture is a progressive fibroproliferative disorder of the palmar fascia that leads to flexion contractures of the digits. It affects approximately 0.6% to 31.6% of the general population, with prevalence increasing with age. While its exact cause remains unclear, it is believed to have a multifactorial etiology involving both genetic and environmental factors. Genetically, it follows an autosomal dominant inheritance pattern more commonly in individuals of Northern European descent. The condition predominantly affects men but can also occur in women, often with a later onset and milder progression. Dupuytren’s contracture is associated with other fibrotic disorders, including plantar fibromatosis (Ledderhose disease) and dorsal hand nodules (Garrod pads). Several risk factors have been identified, including diabetes mellitus, smoking, and chronic alcohol consumption, all of which may contribute to microvascular ischemia and tissue damage. Additionally, the condition has been linked to seizure disorders and chronic liver disease, particularly in patients with cirrhosis. Occupational risk factors, such as repetitive manual labor and prolonged exposure to hand-transmitted vibration, may also accelerate disease progression.
Etiology
Fibroblasts, which are mesenchymal cells responsible for tissue maintenance, play a crucial role in the pathology of Dupuytren’s contracture. The disease progresses through three stages: proliferative, involutional, and residual. In the proliferative stage, fibroblasts are stimulated and differentiate into mature myofibroblasts under the influence of transforming growth factor-beta (TGF-β) and mechanical stress from associated risk factors. As the disease advances to the involutional stage, nodules begin to form, producing an extracellular matrix (ECM) rich in type III collagen. In the residual stage, fibrotic tissue stabilizes as the ratio of type I to type III collagen increases, leading to collagen cross-linking. This results in the formation of fibrous cords, which cause progressive digital flexion contractures. Additionally, the presence of CD3-positive lymphocytes and the expression of major histocompatibility complex (MHC) class II proteins suggest a possible role for a T-cell-mediated autoimmune response in the disorder. In summary, Dupuytren’s contracture arises from fibroblastic proliferation and disorganized collagen deposition, ultimately leading to palmar fascial thickening and contracture formation.
Patients with Dupuytren’s contracture may present with painful or painless lumps in the palm, along with restricted finger mobility and decreased grip strength. As the nodules thicken and fibrous cords form, patients may experience difficulty straightening or spreading their fingers due to flexion contractures. The fourth and fifth digits are most commonly affected, with contractures typically involving the metacarpophalangeal (MCP) joint first, followed by the proximal interphalangeal (PIP) joint, and less frequently, the distal interphalangeal (DIP) joint.
Physical Examination
On physical examination, the Hueston Tabletop Test can be performed. Patients are asked to place their palm flat on a table, and failure to do so indicates a positive test. If contractures are present, the angles at the MCP and PIP joints should be measured to assess disease severity and progression. Grading of Dupuytren’s contracture is as follows: Grade 1 presents as a thickened nodule and band in the palmar aponeurosis, which may progress to skin tethering, puckering, or pitting. Grade 2 presents as a peritendinous band, leading to limited extension of the affected finger. Grade 3 presents as a significant flexion contracture.
Treatment
Although there is no definitive cure for Dupuytren’s contracture, symptoms can be managed through nonsurgical and surgical options. Nonsurgical options include corticosteroid injections, collagenase clostridium histolyticum injections, and needle aponeurotomy. Corticosteroids alleviates symptoms by reducing inflammation while targeted collagenase injections can target and enzymatically degrade the collagen. In needle aponeurotomy, a fine needle is used to precisely cut through the fibrous cord. While this minimally invasive procedure does not remove the cord, a break in the cord allows for improved finger motion. Although more invasive and extensive, a partial palmar fasciectomy removes the abnormal tissue fibrous tissue and cords. Postoperative care includes splinting, wound care, and physical therapy. Emerging therapies include use of anti-tumor necrosis factors such as adalimumab injections to slow disease progression by targeting inflammatory pathways.
Hindocha S, Stanley JK, Watson S, Bayat A. Revised Tubiana’s staging system for assessment of disease severity in Dupuytren’s disease—preliminary clinical findings. EBioMedicine. 2018;36:86-90. doi:10.1016/j.ebiom.2018.06.022.
Zarb RM, Graf AR, Talhelm JE, et al. Dupuytren’s contracture recurrence and treatment following collagenase Clostridium histolyticum injection: a longitudinal assessment in a veteran population. Mil Med. 2023;188(9-10):e2975-e2981. doi:10.1093/milmed/usad075.
Published: January 03, 2025 DOI: 10.7759/cureus.76842
Peer-Reviewed
Cite this article as: Gayibov E, Karim A H (January 03, 2025) A Rapid Review of Adenocarcinoma and Pulmonary Tumor Thrombotic Microangiopathy: A Deadly Duo. Cureus 17(1): e76842. doi:10.7759/cureus.76842
Abstract
Pulmonary tumor thrombotic microangiopathy (PTTM) is a rare paraneoplastic syndrome associated with various adenocarcinomas, most commonly gastric adenocarcinoma. This condition can progressively worsen pulmonary arterial hypertension, leading to acute or subacute pulmonary heart failure and respiratory insufficiency. This paper examines the pathogenesis, clinical presentation, diagnosis, treatment, and prognosis of PTTM. Given PTTM’s poor prognosis, we emphasize treatment strategies. PTTM in adenocarcinoma patients can mimic other pulmonary diseases, causing diagnostic delays. Current PTTM treatment strategies primarily focus on managing the underlying malignancy and addressing thrombotic complications. Anti-angiogenic therapy with bevacizumab and the platelet-derived growth factor receptor antagonist imatinib have shown promise in multiple cases. Further research is needed to develop more effective and targeted therapies for this challenging condition. The precise mechanisms underlying this association remain to be fully elucidated.
Introduction & Background
Paraneoplastic syndromes constitute a diverse group of clinical disorders associated with malignant diseases that can significantly impact patient morbidity and mortality. They are not directly attributable to the physical effects of the primary or metastatic tumor [1]. In these syndromes, malignant cells do not directly cause symptoms related to metastasis; rather, they induce the generation of autoantibodies, cytokines, hormones, or peptides that exert effects on multiple organ systems [2]. It is estimated that paraneoplastic syndromes affect up to 8% of patients with cancer [3]. Table 1 provides a concise overview of commonly encountered paraneoplastic syndromes [4-23].
SCLC, small cell lung carcinoma; SIADH, syndrome of inappropriate antidiuretic hormone secretion
Pulmonary tumor thrombotic microangiopathy (PTTM) is a rare and often underrecognized paraneoplastic syndrome associated with various adenocarcinomas, often linked to gastric adenocarcinoma [24]. Although less frequently observed, breast, lung, and urothelial malignancies have also been linked to PTTM [25]. Post-mortem examinations of carcinoma patients indicate a PTTM prevalence ranging from 1.4% to 3.3% [24,26]. This condition can lead to a progressive deterioration of pulmonary arterial hypertension (PAH), culminating in acute or subacute pulmonary heart failure and respiratory insufficiency. Hence, early recognition and treatment are crucial to prevent irreversible lung damage and complications. First described by von Herbay et al. in 1990 [26], PTTM is characterized by the presence of numerous tumor emboli within the pulmonary microvasculature, leading to microvascular thrombosis and endothelial injury. Later studies have highlighted the critical role of tumor-derived factors in driving hypercoagulability and angiogenesis, as explained in the pathogenesis section.
In this paper, we will examine the pathogenesis, clinical presentation, diagnosis, treatment, and prognosis of PTTM in patients with adenocarcinoma of various origins. Given the poor prognosis associated with PTTM, we will place particular emphasis on treatment strategies. We will discuss the approaches taken in different cases in recent years to inform current best practices, including their limitations and potential avenues for improvement. This rapid review will delve into the current understanding of this rare paraneoplastic syndrome and its potential clinical implications. By reviewing the available literature, we aim to shed light on the pathophysiology, clinical manifestations, diagnostic challenges, and therapeutic options for PTTM.
Review
Methodology
All the studies referred for this rapid review have been searched via the National Library of Medicine (NIH), PubMed, with the free-text keywords “pulmonary tumor thrombotic microangiopathy (PTTM)”, “PTTM AND adenocarcinoma”, “pathogenesis AND PTTM”, “clinical presentation AND PTTM”, “diagnosis AND PTTM”, “treatment AND PTTM”, and “prognosis AND PTTM”. A visual tool Connected Papers [27] and reference manager software Mendeley [28] served for proper citation and access to the studies regarding the abovementioned aspects of PTTM. For this rapid review, we did not specify the time range of studies referred due to insufficiency in number. Our inclusion criteria comprised type I tumor embolism, which is the “classic” or “true” type originating from a distant primary tumor via hematologic seeding with no invasion into vessel walls. Among type I tumor embolism studies, we included ones that specifically focused on the PTTM, either antemortem or postmortem, as a confirmed diagnosis. We disregarded the studies involving type II tumor embolism, which results from a tumor growing into the pulmonary arteries with invasion into vessel walls. The search strategy is summarized in Table 2.
Items
Specification
Date of search
1 October 2024 to 17 November 2024
Databases and other sources searched
National Library of Medicine, PubMed
Search terms used
“pulmonary tumor thrombotic microangiopathy (PTTM)”, “PTTM AND adenocarcinoma”, “pathogenesis AND PTTM”, “clinical presentation AND PTTM”, “diagnosis AND PTTM”, “treatment AND PTTM”, and “prognosis AND PTTM”
Timeframe
No specific timeframe
Inclusion and exclusion criteria
Case reports and reviews were included if they specifically focused on PTTM as type I tumor embolism, the “classic” or “true” type originating from a distant primary tumor via hematologic seeding without vessel wall invasion. Studies involving type II tumor embolism, resulting from a tumor growing into the pulmonary arteries with vessel wall invasion, and mixed embolism were excluded
Selection process
A total of 164 studies were initially identified, of which 55 were ultimately included Author E.G. conducted the literature selection. A.K. supervised the search strategy.
Any additional considerations
Connected Papers [27] and Mendeley [28] served for proper citation and access to the studies
Table 2: Summary of the search strategy for this rapid review
Pathogenesis of pulmonary tumor thrombotic microangiopathy
Associated with mucin-secreting adenocarcinomas, PTTM is a specific type of pulmonary tumor embolism. It is classified within type I tumor embolism, the “classic” or “true” type originating from a distant primary tumor via hematologic seeding without vessel wall invasion [29,30]. In contrast, type II tumor embolism arises from a tumor growing into the pulmonary arteries with invasion into vessel walls [31]. In terms of histopathology, PTTM is characterized by fibrocellular intimal proliferation of small and medium pulmonary arteries and arterioles with the presence of tumor emboli [26,32]. This distinctive feature can be observed using various histological staining techniques, such as Verhoeff-Van Gieson and alpha-smooth muscle actin immunohistochemistry [33,34]. Fibrocellular intimal proliferation involves the growth of cells, primarily smooth muscle cells and fibroblasts, and extracellular matrix within the intima of small pulmonary arteries and arterioles. This leads to narrowing of the vessel lumen. Reactive fibrointimal thickening and occlusion were also revealed in the pulmonary lymphatic vessels and veins in a particular PTTM case [35]. It has also been reported that PTTM is frequently associated with lymphangiosis carcinomatosa, a serious condition that occurs when cancer cells spread to the lymph vessels, causing inflammation and blockage and becoming a predisposing factor to PTTM [26,36]. In PTTM, multiple microscopic tumor cells become stuck to the inner lining of small pulmonary blood vessels. This triggers an inflammatory response, causing the vessel walls to thicken and narrow. Additionally, blood clots form within these vessels, further restricting blood flow. As a result, the lung’s blood vessel network becomes severely compromised, leading to PAH [37,38].
In PTTM, tumor cells not only physically obstruct blood vessels but also release tissue factor (TF), which activates the blood clotting system. They also release inflammatory mediators that promote inflammation and growth factors that stimulate the growth of vessel tissue. This excessive growth can lead to a thickening of the vessel walls, narrowing the blood passage and further hindering the blood flow. Platelet-derived growth factor (PDGF) and vascular endothelial growth factor (VEGF) produced by tumor cells, and versican (VCAN), an extracellular matrix proteoglycan, are considered to be the important factors involved in pulmonary vascular remodeling seen in PTTM [39-41]. Growth factors, particularly transforming growth factor-β (TGF-β), stimulate the expression of VCAN. VCAN binds to growth factors and other extracellular matrix components, creating a local reservoir for these factors [42]. Furthermore, VCAN-hyaluronan aggregates occur in various human lung diseases, including PAH, and provide a permissive environment for arterial smooth muscle growth [41]. These aggregates can be visualized using specific staining techniques with primary antibodies targeting VCAN and hyaluronan-binding protein [43]. Tumor necrosis factor-α, another cytokine released by tumor cells, induces changes in endothelial cell functions, such as upregulation of TF, contributing to the activation of blood clotting system [44].
As previously stated, PTTM is strongly associated with mucin-secreting adenocarcinomas. Mucin production by these tumors likely contributes to the development of PTTM through several mechanisms. Mucinous material can encapsulate tumor cells, forming emboli that travel to the lungs and cause vascular obstruction. Additionally, mucin can stimulate inflammation and damage the vessel walls, further promoting thrombosis. The pro-inflammatory nature of mucin can activate coagulation pathways, leading to thrombus formation [45,46]. While the exact mechanisms are still under investigation, it is clear that mucin plays a significant role in the pathogenesis of this complex disease. Furthermore, circulating tumor-derived, TF-positive microparticles are strongly associated with the activation of blood coagulation, another potential mechanism contributing to the pathogenesis of PTTM that warrants further investigation [47]. Tumor cells express TF and spontaneously release TF-positive microparticles into the bloodstream. Microparticles are small membrane vesicles that exhibit high procoagulant activity. It has been proposed that these circulating tumor-derived, TF-positive microparticles may contribute to the increased rates of thrombosis, including PTTM, as observed in cancer patients [47]. Further contribution to the prothrombotic state can be via a decrease in ADAMTS13 activity. ADAMTS13 is an enzyme responsible for cleaving von Willebrand factor (VWF), a protein involved in blood clotting [48]. Reduced ADAMTS13 leads to an accumulation of large, multimeric forms of VWF. These large VWF multimers are more potent at binding platelets and promoting their aggregation [48,49]. This increased platelet aggregation significantly increases the risk of blood clot formation, contributing to the development of venous thromboembolism and other thrombotic complications in cancer patients, possibly including PTTM.
The interaction between the tumor emboli and endothelial cells via multiple mediators eventually results in the consumption of coagulation factors and platelets, consistent with commonly found laboratory findings, including thrombocytopenia, and disseminated intravascular coagulation (DIC) [25]. Subsequent impaired fibrinolysis in PTTM disrupts the body’s ability to dissolve blood clots in the lungs. This occurs due to an imbalance between clot formation and breakdown, with factors such as increased levels of plasminogen activator inhibitor-1 and decreased levels of tissue plasminogen activator playing significant roles [50]. The resulting persistent blood clots contribute to the development of PAH, right ventricular failure, and other serious complications. The pathogenesis of PTTM is summarized in Figure 1. While growth factors such as PDGF, VEGF, and TGF-β are implicated, the precise molecular pathways driving tumor cell proliferation and invasion in PTTM remain unclear. The mechanisms by which tumor cells arrest in the pulmonary circulation and the role of specific inflammatory mediators in this process need further investigation. The complex interplay of these factors highlights the intricate mechanisms underlying PTTM and emphasizes the need for further research to unravel the precise molecular pathways involved.
Figure 1: Summary of the pathogenesis of pulmonary tumor thrombotic microangiopathy
Clinical presentation and diagnosis of pulmonary tumor thrombotic microangiopathy
Multiple case reports show that the most common symptoms of PTTM include cough, sputum production, shortness of breath, inability to lie down at night, chest tightness, chest pain, hemoptysis, fever, malaise, and wasting. Additionally, fatigue, weight loss, fluid buildup in the legs and ankles, and bluish discoloration of the skin are also reported systemic symptoms [51-54]. In clinical settings, PTTM is primarily a preliminary diagnosis made through a combination of the patient’s medical history, physical examination, echocardiographic and CT imaging, and laboratory tests in patients with cancer. The recognition of PTTM in cancer patients is crucial for several reasons. Firstly, PTTM can significantly worsen the prognosis of cancer patients by accelerating disease progression and increasing the risk of thromboembolic events. Secondly, early diagnosis and appropriate management of PTTM can help alleviate respiratory symptoms and improve quality of life. A diagnosis of PTTM requires a high index of suspicion, especially in patients with sudden onset dyspnea but no radiological findings pointing to pulmonary embolism [55]. Clinicians should be vigilant for PTTM in patients with cancers such as breast, lung, and ovarian, especially those undergoing chemotherapy or with advanced disease. Key symptoms include sudden shortness of breath, chest pain, cough, and hemoptysis [51-54]. Thorough evaluation, including blood tests, chest imaging, and consideration of other diagnoses such as pulmonary embolism and pneumonia, is essential. The challenge in the diagnosis of PTTM can be explained by the low rate of antemortem versus a high rate of postmortem diagnosis, as nearly 80% of identified cases were diagnosed by autopsy [25]. A study by Bak et al. highlights the challenge of diagnosing PTTM. Over 10 years at a tertiary center, they collected 28 cases suspected of PTTM, with only one confirmed histologically [56]. This underrecognition can be further attributed to its nonspecific clinical presentation, rapid disease progression, and the overall rarity of the condition, which often delays consideration in the differential diagnosis.
The clinical presentation of PAH, right ventricular failure, and abnormal laboratory studies including elevation in D-dimer and prothrombin time, the presence of anemia and thrombocytopenia, and DIC should prompt consideration of PTTM [25,57]. Schistocytes may be present in the peripheral blood smear in PTTM, as red blood cells can be sheared by the thickened intima. However, their presence alone is not diagnostic and should be interpreted in the context of other clinical and laboratory findings, such as those associated with thrombotic thrombocytopenic purpura [38]. The elevated D-dimer likely reflects the increased fibrin turnover associated with microthrombi formation in PTTM. Similarly, a prolonged prothrombin time can indicate a consumption coagulopathy, a hallmark of PTTM. Anemia and thrombocytopenia are likely secondary to microvascular thrombosis and platelet consumption in the setting of DIC. The presence of these laboratory abnormalities together with respiratory deterioration suggests PTTM [25,57].
PTTM should also be considered in rapidly dyspneic cancer patients with the presence of PAH on echocardiography without any apparent cause, and with the absence of pulmonary arterial thrombus on chest computed tomography (CT) [57]. Use of pulmonary aspiration cytopathology for antemortem diagnosis has been reported in a few cases [51,58]. For imaging, the use of 18F-fluorodeoxyglucose positron emission tomography/CT has been reported in multiple studies [24,59,60]. Case reports by Tashima et al. [59] and Kamada et al. [60] demonstrated multiple foci with abnormal FDG uptake in both lungs affected by PTTM.
Chronic pulmonary thromboembolism (CTEPH) is a distinct clinical entity that can be challenging to differentiate from PTTM. While both conditions can present with respiratory symptoms, their clinical manifestations and diagnostic approaches differ. In contrast to the acute presentation of PTTM, CTEPH often has a more insidious onset with less prominent respiratory symptoms. Cough, a common feature of acute PTTM, is less frequently observed in CTEPH. CT findings can also be helpful in differentiating the two conditions. In PTTM cases, ground-glass opacities, nodules, mediastinal and hilar lymphadenopathy, and septal thickening are often revealed. In contrast, CTEPH cases may demonstrate mosaicism, wedge-shaped infarcts, organized and calcified thrombus, and enlarged bronchial artery [57]. Additionally, laboratory findings in CTEPH are typically nonspecific and may not reveal the characteristic thrombocytopenia and DIC seen in PTTM [25,61]. Table 3 summarizes the clinical presentation and diagnosis of PTTM.
Feature
Description
Common symptoms
Cough, sputum production, shortness of breath, inability to lie flat, chest tightness, chest pain, hemoptysis, fever, malaise, and wasting
Diagnostic approach
Combination of medical history, physical examination, imaging (echocardiography, CT), and laboratory tests
Importance of early diagnosis
A delay in diagnosis worsens prognosis, increases risk of thromboembolic events, and negatively impacts quality of life
Diagnostic challenges
High rate of postmortem diagnosis, difficulty in differentiating from other pulmonary conditions, and PAH on echocardiography and CT without any apparent cause
Clinical presentation
PAH, right ventricular failure, abnormal laboratory findings (increase in D-dimer and prothrombin time, anemia, thrombocytopenia, DIC), and schistocytes in peripheral blood smear
Diagnostic tools
Pulmonary aspiration cytopathology, FDG-PET/CT. Chest CT may not show typical pulmonary embolism. FDG-PET/CT can reveal multiple lung nodules
Table 3: Summary of the clinical presentation and diagnosis of pulmonary tumor thrombotic microangiopathy
Treatment and prognosis of pulmonary tumor thrombotic microangiopathy
The choice of medication depends on the individual patient and the severity of their condition. Apart from oxygen therapy, the medications used to treat PTTM include those for advanced PAH, such as sildenafil, tadalafil, ambrisentan, bosentan, and epoprostenol [62]. Diuretics such as furosemide and spironolactone help reduce fluid overload, while corticosteroids such as dexamethasone and prednisone have anti-inflammatory effects. Given that PTTM presents with consumptive coagulopathy, anticoagulants should be used with caution. In such cases, low-molecular-weight heparin may be the optimal strategy [63]. In pulmonary embolism, the pathology is primarily caused by the activation of the blood coagulation cascade, but in PTTM, fibroproliferative changes in the vascular lumen arising from TF release are the prominent causes. Therefore, while anticoagulant therapy may be effective for pulmonary embolism, it cannot improve PTTM. In the case of right heart failure, intravenous diuresis, inotropic support, and pulmonary vasodilator therapy should be considered [54]. A multidisciplinary approach involving pulmonologists, oncologists, and other specialists is essential for the optimal management of PTTM patients. A patient-centered approach, which includes timely supportive care and symptom management, can improve quality of life and alleviate symptoms.
At present, PTTM management lacks a consistent, evidence-based approach due to the condition’s rarity and rapid progression, which frequently leads to late diagnosis and intervention. Almost all patients with PTTM die within a week of the dyspnea onset due to progressive PAH, subacute right heart failure, or sudden death [53,64]. The rarity of PTTM poses significant challenges to research, including small sample sizes and difficulty in recruitment for clinical trials. While anti-inflammatory therapy with corticosteroids has been frequently utilized as a potential treatment strategy for PTTM, its efficacy remains uncertain [53,65-67]. A case report by Miyazaki et al. demonstrated a temporary improvement in lung function and right ventricular pressure overload following corticosteroid administration [53]. However, the patient ultimately succumbed to respiratory failure, highlighting the limitations of current therapeutic approaches and the need for further research to identify effective interventions for this challenging condition. Other studies similarly reported the ineffectiveness of anti-coagulants and corticosteroids [65-67].
Clinical reports suggest that bevacizumab may be a valuable therapeutic option for patients with PTTM, especially when used in conjunction with other therapies. Higo et al. presented a case study of a colorectal cancer patient exhibiting PTTM who underwent a combination therapy involving imatinib, a PDGF receptor antagonist, bevacizumab, a VEGF receptor inhibitor, and the chemotherapeutic agents S-1 and cisplatin [68]. Following this treatment regimen, the patient exhibited a significant improvement in symptoms without experiencing a deterioration of PAH. However, 12 months post-treatment, the patient succumbed to respiratory failure secondary to an influenza infection. Despite this outcome, the authors posit that the molecular-targeted drugs employed in the therapy were efficacious in managing PTTM based on the patient’s clinical trajectory [68]. Kotake et al. reported a significant improvement of PTTM with lung adenocarcinoma in terms of PAH, respiratory symptoms, and other outcomes after bevacizumab treatment combined with paclitaxel and carboplatin [69]. Taniguchi et al. reported a similar improvement in uterine cancer-induced PTTM after successful treatment with platinum-based chemotherapy and bevacizumab [70]. These case studies suggest that bevacizumab, in combination with other therapies, may be a promising treatment option for PTTM, especially when used in conjunction with targeted therapies. Bevacizumab therapy can be associated with adverse effects. The most common side effect is hypertension, which requires regular blood pressure monitoring and effective management with antihypertensive medications. Proteinuria, thromboembolism, impaired wound healing, and bleeding are other clinically encountered side effects [71]. In more severe cases, a minority of patients may develop thrombotic microangiopathy (TMA). Bevacizumab-associated TMA, along with other drug-induced TMAs, is currently an indication for drug discontinuation due to poor prognosis, including acute kidney injury often requiring dialysis and progression to chronic kidney disease. Most cases, however, improve after discontinuation of bevacizumab [72].
Imatinib has demonstrated promising results in addressing complications associated with PTTM, as evidenced by several case studies. The efficacy of imatinib in treating a patient with PAH associated with PTTM has been demonstrated by the case study of Ogawa et al. [73]. Following imatinib therapy, the patient experienced a dramatic reduction in PAH, enabling successful weaning from percutaneous cardiopulmonary support within a 20-day timeframe. Based on these findings, the authors suggested that imatinib may be a viable therapeutic option for alleviating PAH arising from PTTM [73]. Kimura et al. [74] reported a case of a breast cancer patient with PTTM who experienced a dramatic improvement with bevacizumab therapy. The patient received paclitaxel and bevacizumab for one year, successfully controlling the condition and extending their survival to one year and eight months. This case highlighted the potential efficacy of bevacizumab in managing PTTM associated with breast cancer [74]. Another case study reported that bevacizumab combined with pemetrexed significantly improved lung adenocarcinoma-induced PTTM respiratory dysfunction [52]. Yoshikawa et al. also reported a case of PTTM associated with metastatic breast cancer, which exhibited a significant improvement of respiratory dysfunction and PAH after imatinib was administered [75]. Similarly, imatinib dramatically alleviated the PTTM induced by gastric cancer in another case report by Kubota et al [76]. These findings underscore the potential of imatinib as a targeted therapy for PTTM. Yet still, imatinib can cause a range of cutaneous side effects, along with fever and diarrhea. A maculopapular rash is the most common. For many patients experiencing intolerable side effects, temporarily reducing the dose can help resolve the issue [77]. Furthermore, while both bevacizumab and imatinib are approved medications, access can be challenging due to factors such as cost, insurance coverage, and availability. Similar to bevacizumab, imatinib can also result in drug-mediated TMA, as reported in two cases [78]. Therefore, the administration of bevacizumab and imatinib should be considered carefully, taking into account the potential for drug-mediated TMA. Table 4 summarizes the referred studies regarding the treatment and prognosis of adenocarcinoma-induced PTTM.
Successful improvement in chest CT findings, respiratory symptoms, DIC. On the second day, dyspnea improved, and The patient could complete walking exercises. Cough was gradually relieved, without any further hemoptysis, together with significantly improved fatigue, sleep, food intake, and mental and physical status
Successful improvement in PAH, respiratory symptoms, and other outcomes. On day 10, oxygen saturation rate was improved to 95%, and she was discharged after recovery was confirmed
Patient’s respiratory status and radiological findings improved concomitantly with a reduction in the size of the tumor. The patient recovered well from respiratory failure and her condition has improved, even six months after the end of treatment
Significant decrease in mean pulmonary arterial pressure five days after imatinib administration. The patient was discharged and lived without symptoms of PAH until her death due to systemic metastasis of carcinoma
Table 4: Summary of referred studies regarding the treatment and prognosis of PTTM
These case studies suggest that targeted therapies, such as bevacizumab and imatinib, may offer promising therapeutic options for patients with PTTM. While further research is needed to establish definitive treatment guidelines, these studies provide valuable insights into the potential benefits of these agents in managing PTTM-related complications. It’s important to note that the referred studies are case reports. While valuable for generating hypotheses and describing rare occurrences, case reports have inherent limitations that should be considered. These limitations include limited generalizability, lack of a control group, potential for bias, limited statistical power, and a retrospective nature. Further research, such as larger observational studies or randomized controlled trials, is often needed to confirm the findings and draw more definitive conclusions.
Future research should focus on identifying additional biomarkers that can predict patient response to these therapies and developing novel therapeutic strategies that target the underlying pathophysiological mechanisms of PTTM. These mechanisms may include the activation of coagulation cascade and release of inflammatory mediators, fibrocellular subintimal proliferation, and smooth muscle cell colonization [28]. Several potential biomarkers have been associated with PTTM, including VEGF, PDGF, osteopontin, and TF [35]. These biomarkers are involved in pathways that contribute to the pathophysiology of PTTM, including angiogenesis, coagulation, and cellular proliferation. Further research is needed to validate their utility in clinical practice and to explore their potential in early diagnosis and targeted therapy for PTTM.
Conclusions
In conclusion, the association between adenocarcinoma and PTTM presents a significant clinical challenge. Current treatment strategies for PTTM in adenocarcinoma patients primarily focus on managing the underlying malignancy and addressing thrombotic complications. Anti-angiogenic therapy bevacizumab and a PDGF receptor antagonist imatinib have shown promising results in some cases.
Future research should focus on the early detection of PTTM in adenocarcinoma patients, understanding the molecular mechanisms underlying the association between these two diseases, and developing innovative therapeutic approaches that target the aforementioned specific pathophysiological processes involved. By advancing our understanding of PTTM in adenocarcinoma, we can improve patient outcomes and ultimately save lives.
Tran K, Coyle K, Jabr MF, et al.: Discussion. Drugs for Pulmonary Arterial Hypertension: Comparative Efficacy, Safety, and Cost-Effectiveness [Internet]. Tran K, Coyle K, Jabr MF, et al. (ed): Canadian Agency for Drugs and Technologies in Health, Ottawa; 2015.
By Dr. Arnav Kumar MD, MSCR Interventional Cardiologist HCA Medical Center Hospital Houston, Texas
87 year old extremely pleasant, active woman was sent to us for complex LM PCI . She has distal left main 70% disease, ostial LAD 70% disease, calcific 90% disease of the proximal high Obtuse marginal artery and 99% Proximal LCX disease.
The left main itself is very long and anomalous. We anticipated challenge in delivering equipments across the retrofelxed LCX. Additionally, she has distal RCA disease . She was felt to be too high risk for CABG due to advanced age We were able to cross the ostial LAD – lesion using a sion blue wire. We were able to cross the high OM lesion using a minamo wire.
Crossing the 99% very calcified proximal left circumflex lesion proved challenging. However, we were able to cross it using Fielder XT.
Retroflexed LCX, anomalous long LM have high risk of stent dislodgment left main dissection and wire dislodgement.
The plan was to do double cush- however, no stent would go across the LCX lesion. We first pre dilated LM, LAD, LCX, ON lesions. We did encounter challenges in delivering balloons into LCX. After Predilation, we placed a stent in the OM and crushed it with a ballon placed in LM-LCX. However we faced extreme difficulty in placing stent in the LCX-LM. Finally, we had to take out both the OM and the LAD wire and were successful in delivering the stent across the LXC lesion using guideliner support (advancing the guideliner in to the LCX). After deploying the stent In the LM-LCX, we post dilated with an NC balloon.
We quickly crossed back into the the LAD – ie switched to a coullote technique..
Final angiograms demonstrated excellent stent expansion, no edge dissection and no geographic miss.
Impella was taken out at the end of the procedure and LFA was perclosed. Patient underwent PCI of RCA two days later and discharged home In great spirits
Extremely retroflexed LCX – showing that all stents started prolapsing- unable to deliver; Had to sacrifice LAD, OM wires to advance a guideliner into the LCX… and hence was able to place a stent into the LCX-LM. However this meant that we had to change to coullote technique; Placed a stent in the LAD – LM
Then simultaneous kissing balloon inflation of the LAD-LM-LCX
By Paulina Maldonado Universidad De Durango, Chihuahua, Mexico Houston, Texas. Amin H. Karim MD Baylor College of Medicine and Methodist Institute of Academic Medicine, Houston, Texas
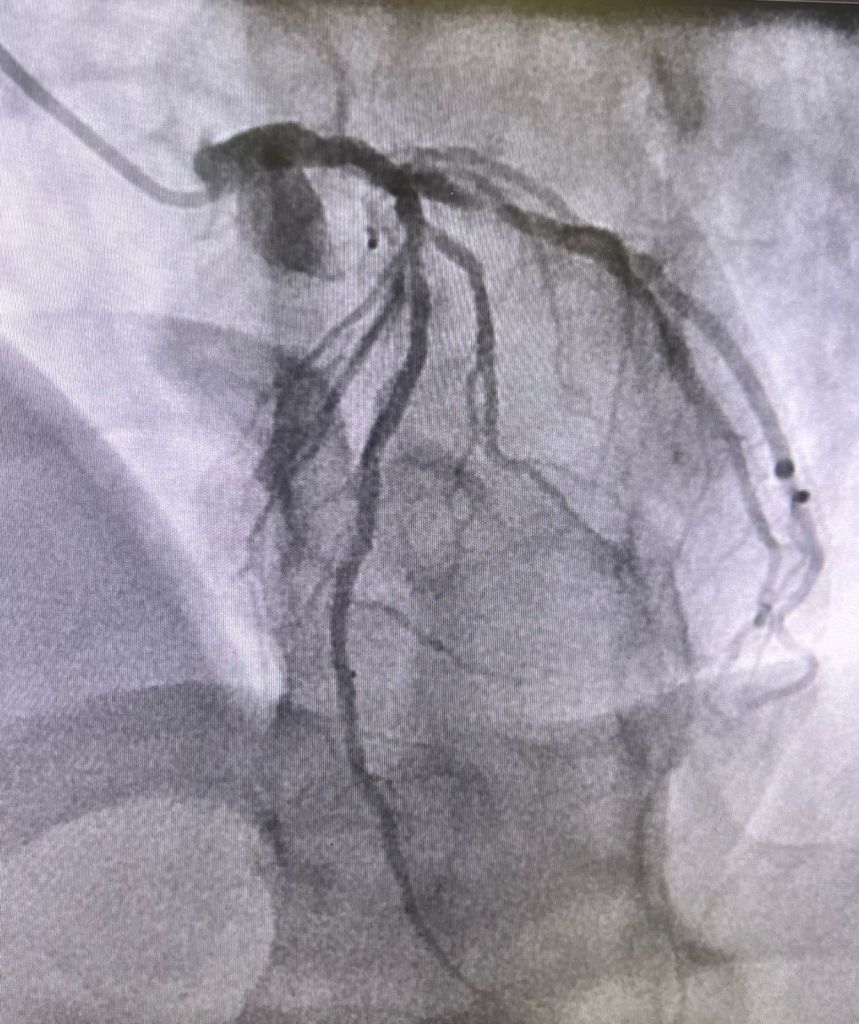
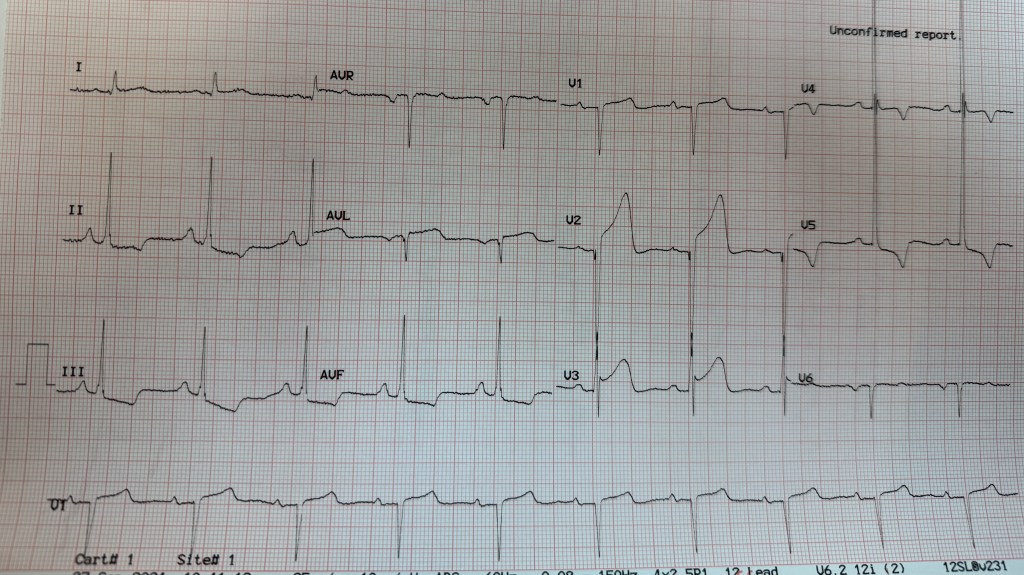
A 65 year old patient presented, disabled from old cerebro vascular accident causing flaccid left sided hemiplegia with contractures, admitted to hospital for change of mental status; he developed hypotension; EKG showed ST elevation in II, III and aVF as well as V3V4V5 diagnostic of inferior wall myocardial infarction with lateral extension.
He was rushed to the cath lab where cardiac catheterization showed what looked like “normal coronary arteries”.
His high sensitivity peaked at 1200. He was treated with intravenous heparin and beta blockers; he remained hemodynamically stable and was discharged.
Myocardial Infarction with nonobstructive coronary atherosclerosis
Although the occurrence was initially reported about 80 years ago a very small number of patients are found to have MINOCA.
The term MINOCA is reserved for patients with elevated troponin associated with myocardial ischemia at presentation and should not include disorders with non ischemic elevated troponin.
It is important to mention and reiterate that MINOCA should not be considered a final diagnosis but rather a working one that requires further testing.
Epidemiology
The incidence of MINOCA varied from 1% to 15% and roughly 6% of all Acute Myocardial Infarction cases.
Younger (18-55)
Female
lower prevalence of hyperlipidemia
⅓ presented with ST segment elevation of myocardial infarction
Pathogenesis:
MINOCA is heterogenous and can be divided into coronary, cardiac and extra cardiac causes. Ischemia happens during a temporary suspension of blood flow to the myocardium and it takes place in the epicardial arteries or the microvasculature.
Coronary
Cardiac
Extra cardiac
plaque rupture or erosion
Myocarditis
stroke
coronary spasm
Takotsubo syndrome
pulmonary embolism
spontaneous coronary artery dissection
cardiomyopathies
sepsis
coronary embolization
cardiac trauma
renal failure
coronary microvascular disorders
tachyarrhythmias
hypoxemia
Risk factors:
Associated with Long term major adverse cardiovascular events after MINOCA including ST segment elevation on a presenting Electrocardiogram
older age
reduced left ventricular ejection fraction
diabetes mellitus
hypertension
tobacco use
prior Myocardial infarction
Stroke
peripheral artery disease
chronic obstructive pulmonary disease
chronic kidney disease
lower total cholesterol
Peak troponin
Depression at the time of MINOCA
Signs and Symptoms:
Chest pain/chest pressure / chest heaviness
Nausea
jaw, neck or upper back pain
pain or pressure in the lower chest or upper abdomen
shortness of breath
fainting
indigestion
fatigue
Diagnostics:
Requires a comprehensive diagnostic workup. Is the first line diagnostic tool to detect non obstructive epicardial coronary arteries (less than 50% stenosis) in the setting of an Myocardial Infarction.
Imagining modalities are vital in diagnosing and identifying the underlying mechanisms of MINOCA.
Coronary intravascular imaging
With Intravascular Ultrasound 40% cases and Optical Coherence Tomography 50% cases is essential to diagnose plaque disruption.
It should be performed at the time of coronary angiography for Acute Myocardial Infarction in all 3 major epicardial arteries.
Cardiac Imaging
Transthoracic echocardiography used in the assessment of cardiac function after a MINOCA. It can be used in the diagnosis of Takotsubo cardiomyopathy and non ischemic cardiomyopathy specifically to demonstrate recovery of left ventricular function.
Transesophageal echocardiography can be used when coronary embolism is suspected.
Cardiac Magnetic Resonance Imagining (CMRI) provides a diagnosis in 74-87% of all MINOCA patients.
Subendocardial (or transmural) pattern of myocardial edema, inflammation or fibrosis is suggested of ischemic Myocardial Infarction.
Epicardial pattern is suggestive of non ischemic Myocardial Infarction.
Echocardiogram can be used to diagnose Takotsubo cardiomyopathy and non ischemic cardiomyopathy, but CMRI can only be used to detect myocarditis.
Myocardial perfusion quantification with adenosine or regadenoson can be used to diagnose coronary microvascular dysfunction non invasively.
The timing to perform a CMRI is important; it should be completed as close to the acute myocardial infarction as possible. CMRI carries not only diagnostic value but prognostic value as well.
Multimodality approach
OCT and CMRI together resulted in a diagnosis in 85% of the cases whereas Optical Coherence Tomography alone was only 46% and Cardiac Magnetic Resonance Imagining 74%.
Treatment
It should me customized to the underlying diagnosis:
Meds
Underlying diagnosis
Aspirin and High intensity statins
Plaque disruption
dual antiplatelet therapy by adding ticagrelor for less than 1 month
Plaque disruption not undergoing stenting
Beta blocker and renin angiotensin system inhibitors
left ventricular dysfunction
Long acting calcium channel antagonist (dihydropyridine and nondihydropyridine)
MINOCA patients secondary to epicardial coronary vasospasm
nitrates can be added to calcium channel antagonists
refractory variant angina
antithrombotic agents
coronary embolism or thrombosis
targeted therapies
underlying thrombophilia
conservative management (avoiding increased risk of complications with intervention)
spontaneous coronary artery dissection
Percutaneous coronary intervention
STEMI, cardiogenic shock, ongoing ischemia
aspirin, beta blocker, statin and renin angiotensin system
spontaneous coronary artery dissection (should be assessed based on individual risk factors
antianginal treatment with b blockers, calcium, channel antagonists and ranolazine
Chest pain
MINOCA mimickers
Heart failure
mechanical circulatory support
progressive circulatory failure
resolves in most patients within 2-4 weeks
Myocarditis, but if they develop arrhythmia and persistent cardiac dysfunction medical therapy should be administered.
antivirals and immunosuppressives
underlying etiologies
Prognosis:
Short and long term mortality
At 1 year follow up, MINOCA mortality is 2 to 5%.
Among individuals 65 and older the risk of adverse outcomes is higher 12%
Possible Reinfarction
only occurs in 1.3 to 2.6% of patients at 1 year and 7.1% at 4 years.
Quality of life
Identified factors that increase the risk of Major advance cardiac event:
older age
hypertension
smoking
reduced ejection fraction
chronic obstructive pulmonary disease
elevated creatinine
cancer
elevated CRP
Requires further investigation that may require longer hospitalizations. It is commonly found that Myocardial Infarctions is missed in women due to non classic presentations such as shortness of breath, dizziness, nausea or unusual fatigue. Patients with MINOCA do present with recurrent chest pains without myocardial infarction.
Literature Cited:
Tamis‐Holland, J. E., & Jneid, H. (2018). Myocardial Infarction With Nonobstructive Coronary Arteries (MINOCA): It ‘s Time to Face Reality! Journal Of The American Heart Association, 7(13). https://doi.org/10.1161/jaha.118.009635
Takahashi, J., Onuma, S., Hao, K., Godo, S., Shiroto, T., & Yasuda, S. (2023). Pathophysiology and diagnostic pathway of myocardial infarction with non-obstructive coronary arteries. Journal Of Cardiology, 83(1), 17-24. https://doi.org/10.1016/j.jjcc.2023.07.014
Yildiz, M., Ashokprabhu, N., Shewale, A., Pico, M., Henry, T. D., Quesada, O. (s. f.). Myocardial infarction with non-obstructive coronary arteries (MINOCA). Frontiers In Cardiovascular Medicine, 9. https://doi.org/10.3389/fcvm.2022.1032436
De Oliveira, L. L. H., Correia, V. M., Nicz, P. F. G., Soares, P. R., & Scudeler, T. L. (s. f.). MINOCA: One size fits all? Probably Not—A review of etiology, investigation, and treatment. Journal Of Clinical Medicine, 11(19), 5497. https://doi.org/10.3390/jcm11195497
Talking JSKBT ( jailed semi inflated kissing balloon technique ) We did multiple JSKBTs here. Zameer our Pakistani fellow made these images.
Patient had CP/ NSTEMI in a decent sized town 100 miles away. Which has good sized hospital and interventional cardiologist’s and PCIs / primary etc are done. No CABG onsite. Cardiologist did angio for intervention purposes. Saw the anatomy Calcified distal left main, Ostial/ prox / mid LAD, 90% tight ramus, 90% bifurcation LCX/OM1 and CTO RCA. EF 30% with severe MR ( so even poorer forward flow / and overestimation of the LV function due to MR).
Referred to our surgeon. He said he can ! But very high risk. ( calcified aorta not. Great candidate to put on heart lung bypass / previous EVAR, Poor LV function, ) so referred to one of our colleagues – who said very high risk PCI. Referred back to surgery. Nothing happened. Meanwhile patient having symptoms. So the primary interventional cardiologist from the other city called us. Was going to need 3 to 4 wires with multiple balloons at a time. So needed an 8 French guide so did do single access Impella. Also deliberately took a short JL 3.5 guide ( which obviously has low support ) so we can sit outside this shortish left main and work
LAD was quite retroflex so you can appreciate flipping of hydrophilic coated wire with >120 bend with microcatheter assistance. Later changed to wiggle wire; So onwards LAD was started. Calcified, retroflex and quite some tortuous so IVUS was done after first run of 2.5 pre-dil; Still there was IVUS malfunction in mid autorun so predilated with 3.0 balloon and ReIVUS Heavy more than 270 degrees calcium is there; Further vessel preparation was done with 3.0 IVL all the way upto LMS
This is tight LCX and tight OM1. Kissing balloon inflations and then stent in LCX and JSKBT is OM. Notice 4 wires in there. Pretty good result. OM Latium looks really good. IVUD of LCX stent good. Did POT of the proximal LCX with NC balloon; This is the long 3.0 x 48 synergy xl. Extending from mid LAD to left main and have 3.0 x 15 balloons as JSKBTs in Intermediate and LCX
Couldn’t get the IVUS to distal edge to see if it is dissection or spasm. These new Hi Def boston IVUS shafts are flimsy and you push them and they get bent. Used three different catheters during this long intervention. Cuz it would get stuck in calcium and then either stop working or the shaft get bent. So images look like distal edge dissection. Placed a 2.5 mm shirt stent. Looked good after wards
IVUS from LAD stent back to left main. Had also done a 4.5 x 6 mm short NC balloon POT for left main. ( size mismatch between left main and LAD)
Of course without Impella. Wouldn’t have been able to do these. With occluded RCA and EF 30% with severe MR. I was getting flat line pressures with IVL and Thenleft main stenting with JSKBTs
By Dr. Arnav Kumar MD MSCR Interventional Cardiologist HCA Medical Center, Houston, Texas
Pt was 61 active pt – was sent from another hospital Late presentation STEMI The impella they had placed clotted his right leg. Then he had 23 min code for VFiB arrest – I placed LFA/LFV ECMO bedside. He had right leg ischemia from the prior placed impella. So I and vascular surgery switched to 5.5 impella via left subclavian. So only two options for pci access were either radial or stick the ECMO circuit. Angiogram with 100% LAD and LCX, 99% calcific LM. We preformed ivus guided bifurcation PCI of LM-LAD-LCX after rotational atherectomy of the LM – LAD. Also reconstructed the whole LAD. Was able to do all radial fortunately.
A Panel Discussion Between Practicing and Experienced Cardiologists on How to Tackle Risk Assessment in Asymptomatic People .
The case presentation and the comments that follow were interchanged on our WhatsApp groups APCNATeam in November 2024. This discussion presents an example of how experienced practicing cardiologist, faced with real life patients, navigate the findings on trials and papers and come to conclusion of what to tell the patient and how to proceed with the next preventive or therapeutic step. Please excuse any errors or omissions and will be happy to correct since the readers are themselves the Editorial Board. (Amin H. Karim MD)
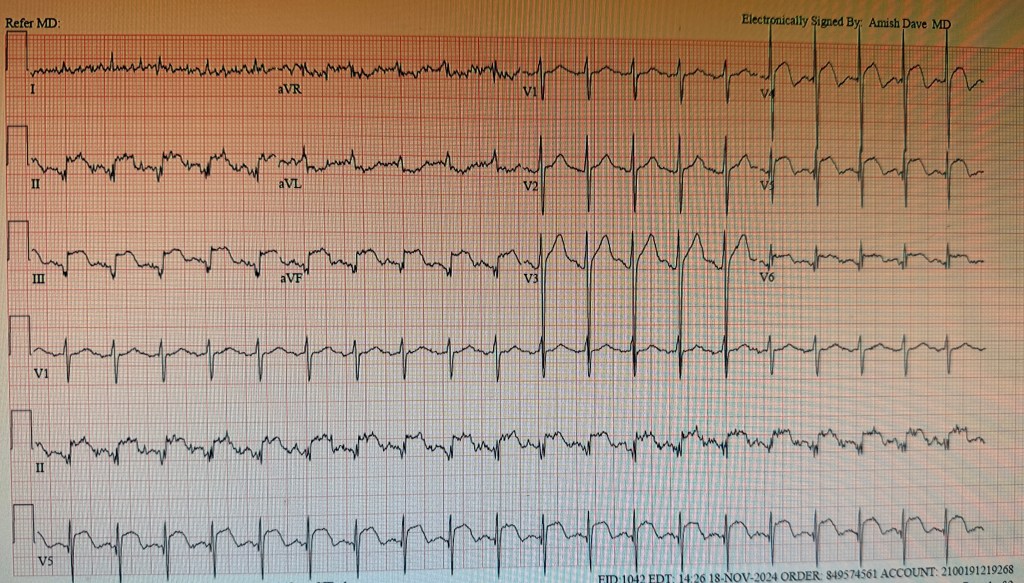
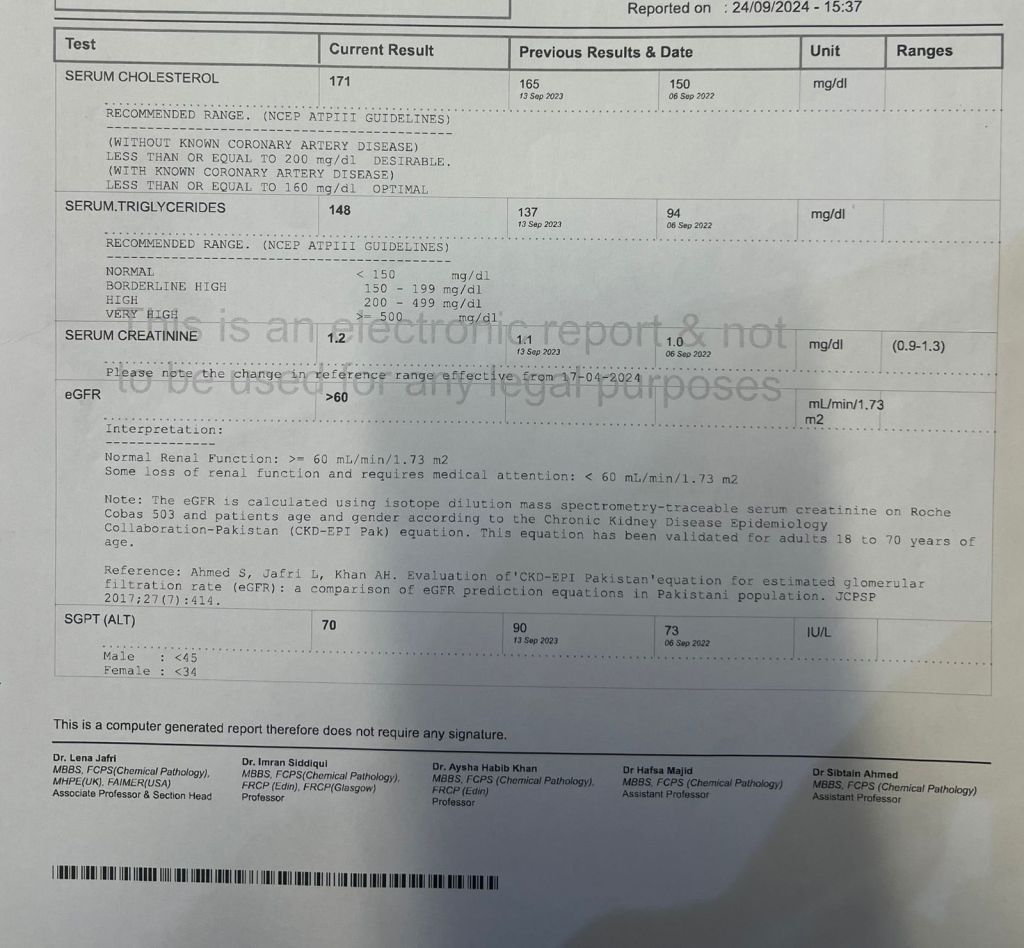
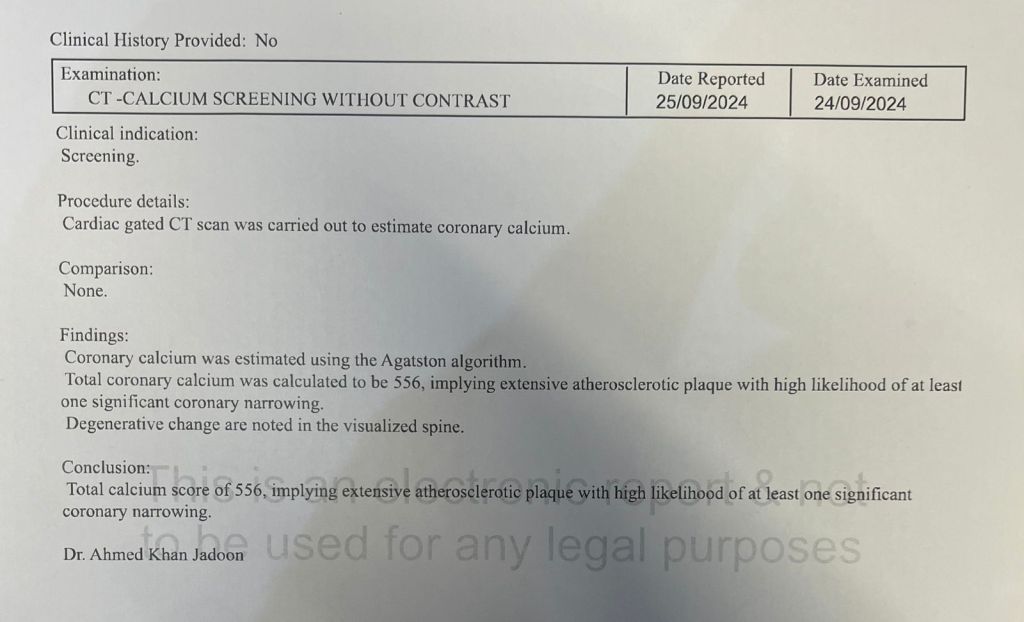
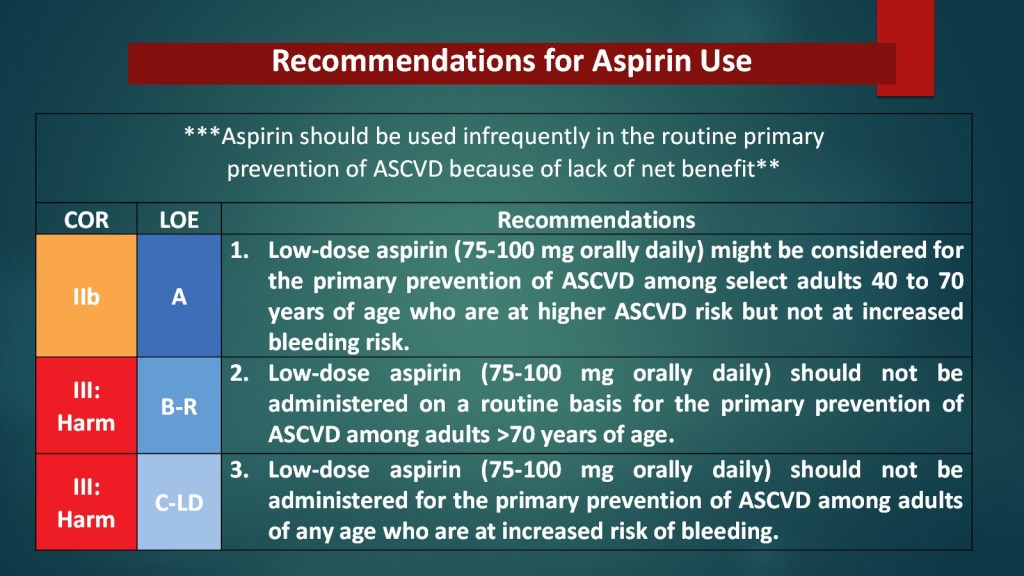
Dr. Bashir Hanif Need opinion on a 45 year old with positive family history of premature CAD. Asymptomatic. Very active, brisk walk n jog 45 minutes 6 days a week without symptoms. CAC n Lipids are given below. What would you do next? Cath? Stress test? Or just Aspirin n high dose statins?
Abdul Hakeem Where is the bulk of the calcium? If it’s a prognostically imp territory then I would get exercise MPS for further risk stratification. Agree with HD statin bring LDL<50 perhaps EPA Salman Arain I had the same question @Dr.Basheer Hanif – what is the distribution of calcium? 550 distributed over three vessels is less concerning than 350+ in the LM and proximal LAD. In the latter case, I may offer a stress test. Also, if the patient has a family history of premature CAD, then it may be reasonable to do a stress test.
Maryam Moten
Hussain Khwaja I would do ASA and high dose statin to bring LDL between 25-50 Question is what we are going to do if stress test comes abnormal ? Basheer Hanif That was my problem too as this was the only report apparently they gave which doesn’t give distribution of calcium. He is completely asymptomatic despite heavy exertion. Abdul Hakeem So how does calcium scoring help in a very active asymptomatic person? Just creates a very pesky conundrum Khurram Nasir Preventive Management my friend, think beyond stenosis and intervention Muhammad Saad it can help to emphasize use of statins in asymptomatic patients Khurram Nasir Ldl below 55 Check Lpa if high family screening ASA SBP below 130 GLP1RA if diab pre diab Further emphasize on diet and lifestyle Abdul Hakeem I have heard that and I’m sure there is some piece of evidence that it modifies human behavior but the consternation it causes seems to be its overwhelming impact! Khurram Nasir Few thoughts : Make sure they’re not capturing any MAC
paradoxically the more number of vessels involved the more risk (prognostically) vs the more rationale thinking that if higher in one vessel possibly higher risk of stenosis or future risk
the relationship of high cac is not correlated with the stenosis in the same vessel, actually u may find often in the other with less score
the issue is more distributive cac more turbulence in flow and more risk beyond plaque burden and rupture risk
despite higher risk, majority don’t have event so no good way to assess who specifically is more at risk
stress test not a bad idea in these uncertain cases hopefully pak Sehat with cac and CCTA in young Pakistanis will tell us what it means so kudos to bashir on leading the way
There is now huge body of evidence, actually, there is a meta-analysis from our group and JCC imaging that higher cac modifies, patient lifestyle, behavior, and attendance, and as well as physician behavior on prescription patterns
Also, as thought, from rationale thinking that it may increase anxiety and concerns, apart from few anecdotal cases, actually the evidence suggest otherwise
I see these patients all the time, it is how you message to them, that is great that you found out this,rather than waiting for an event to happen, and we have simpler an easier way to significantly modify the risk
Abdul Hakeem Calcium score (in hugely asymptomatic)= demaagh me keera. The pt will find himself a Cardiol who will be more than happy to cath and stent him ( to prevent events Khurram Nasir I believe you; Well, just because there are bad practices, and some of these arguments have been made by long-term skeptics like David Brown even in the US, doesn’t mean that we stop doing the right thing
it means we start educating not only the patients, but also Cardiology community on what the best practices are
This is like saying we should stop screening for hypertension, because most of cardiologist will start on clonidine and may cause more harm
The same argument it’s gonna be made for anything For deemagh me keera means more patient discussion and education and that means spending more time at the patient, unfortunately, that doesn’t exist much in most place even beyond Pakistan, and maybe that’s what we need to do, so we have more patient centric approach and care.. And btw asymptomatic doesn’t mean the person is not high risk for MI not only long term but also short term Can’t think of any good rationale why the pt and pts physician wouldn’t want to know about so actually one can mitigate this totally preventable catastrophic complications and downstream issues like revascularization Abdul Hakeem I can’t agree more. I’m just saying unless we have solid evidence that “screening ca scores” in healthy asymptomatic individuals alters long term outcomes incrementally to usual practice we should be selectively doing calcium scores particularly in prevention rebellious pts Khurram Nasir First of all, this is old school, and things have changed: Let me help, explain, also, we need to put yourself in the patient’s shoes and ask ourselves whether we are better off in making a guess or knowing the actual risk and personalizing management accordinglyly
Cac test is no longer a screening test but more of a decision aid to guide risk and management, screening means that you do it for a person who is not candidate for a therapy, you find disease, intervene, and see if it improves. Here cac is also used for a lot of individuals who are already candidates for therapy, is to guide whether they need it or not and what intensity, so completely different philosophy.
well proven to outperform any guesstimation approaches that you and Ion and others use in the clinic, and by the way, none of them have been tested in any randomized trial that using them improves outcome.. also by the way that I said I would be in a study that seeing a cardiologist improves outcome so maybe we can take everything with a grain of salt
as far as a pure screening approach and outcomes this concert there is a large study in Denmark, which is ongoing, and in the interim analysis has shhkwn 11% reduction in MI and stroke in the entire population, and three specified analysis, almost 11% all cosmetology reduction, and younger individuals Abdul Hakeem Thanks for the insightful comments khurram bhai. Always very scholarly and encyclopedic! Syed Iqbal Rahmatullah Repeat CAC to know the distribution or get the scan film to review. High dose statin (goal LDL 30 to 40) Aspirin Lp a Stress echo regardless of distribution Life style adjustment. (Particularly dietary, HbA1c, BMI)
I had a similar patient yesterday, asymptomatic, played squash 5 days a week, and had very low LDL, CAC 350, pakistani recently retired anesthesiologist, age 62, visiting his son here. No other risk factors. SE showed anterior and inf wall hk, Rest echo 65%ef, post exercise 45%. LHC showed discrete lesions but diffuse 3 vessel disease, extensive but good targets. Scheduled for cabg next week. Farhan Katchi I’ll just add that i use cac, as informed largely by Khurram’s body of work, and it has strengthened patient trust, buy in, compliance, and in my 7 years IMO better outcomes. My patients are more motivated to lose weight, eat better, exercise, and engage in escalating up medical preventative therapy when they know and understand the cac score concept (I show them the images in clinic on the screen so it’s concrete and not abstract). I have started to use LP(a) and ApoB in the same way that I use cac scores for risk adjudication, especially in women and the young where a cac of 0 may not tell the full longer term preventative story. Bashir Hanif:
Syed Fazal: Great discussion! Now at the end of discussion, looks to like need one stent in type A lesion in mid cir, and all the above recommendations, for secondary treatment! Now he will need more anti platelets med for stent! Bashir Hanif: So who will put a stent and who would treat it medically. He is completely asymptomatic. It’s not a prognostic lesion! Syed Arman Raza Academic answer (in my view): no stent. Medical mgmt. Real world: stent + medical mgmt Sabha Bhatti Has he had functional testing ?If there’s ischemia in that territory you could consider stenting Bashir Hanif: You know functional study is going to be low risk and we are not going to change his prognosis/ risk of MI or mortality by putting a stent!! Sabha Bhatti: Yes but … Potentially that’s the bridge between academic and real world answer .. you have another justification for not stenting if there’s no ischemia Bashir Hanif: There will be ischemia. I can tell you what functional test is going to show. He jogs for 45 mins without symptoms. So it’s probably going to be medium size mild intensity ischemia at high work load. Will you send him to Hakim for stenting with this report? Sabha Bhatti: No one can do 45 min on a Bruce . Infact 16 min and few sec is the max I’ve seen . It helps to see symptoms , ECG and ofcourse vitals with exercise. No stent for now . Avoid oculostenotic reflex Bashir Hanif: I didn’t say 45 mins Bruce. I said jogs n brisk walk for 45 mins. I advised him medical treatment. No stent Ata Qureshi This is a non prognostic, low risk lesion and I would manage it medically. Syed Iqbal Rahmatullah Bashir, was FFR done on left circ lesion? What was the rationale for doing cath, to begin with? Bashir Hanif: My point is it’s a non prognostic lesion pt is asymptomatic. Even if it had shown some ischemia or FFR was positive, in asymptomatic pt , would stenting change the risk of future MI or mortality?? I believe in CCS but if pt is symptomatic on GDMT or it’s a LM or may be Ostial LAD I would go for invasive approach and revasc. options. I don’t know about you and Hakeem but I had to relearn medical management of CCS when I moved back as lot of patients refuse to go for Revasc ( even LM n 3 VD ) and they are doing fine on medical management for years now. So as you said we need to resist oculostenotic reflex as much as possible!!( Disclaimer: I am an Interventionalist) My 20 years of experience in Pakistan tells me Medical management can do wonders if done appropriately with belief!! Abdul Hakeem One our fellow intv cardiologist has classified this very well. Reasons for PCI in SIHD if I can’t do it then GDMT If I don’t do it someone else will medical therapy until I return from vacation Syed Fazal I think most of us IC do lot more stents without evidence of mortality benefit. Definitely there are regional differences for many other obvious reasons in different countries. And as I said there is no consensus in this type A lesion. Definitely in board exam don’t even think about stenting at this lesion! Farhan Katchi In cases of high cac, if I suspect LM or 3VD, I will Cath or CCTA to define anatomy for cabg referral. EXCEL and NOBLE and guidelines support revasc of this disease with cabg on account of its survival benefit even in asymptomatic patients. Now the ven diagram of asymptomatic and severe LM and significant 3VD is probably tiny especially if you consider 3V ischemic rather than anatomic disease and verify “asymptomatic” status on a treadmill Haris Riaz: I haven’t had a chance to follow this interesting discussion but ISCHEMIA trial frequently gets cited [sometimes even by people who haven’t actually read the full text or gone through the supplementary materials from nejm]. It might be interesting to note that: One fifth patients in the conservative arm underwent revascularization There are many other important limitations that need to be kept in mind before applicability. The trial [like COURAGE] reaffirms that medical management is effective in stable patients with stable symptoms compliant with GDMT. Approximately one third of patients in ISCHEMIA had no angina in the last month before enrolment. 15% patients in ISCHEMIA had no objective evidence of ischemia on core lab assessment One fifth patients in the invasive arm didn’t undergo revascularization
Amin H. Karim MD Institute for Academic Medicine Houston, Texas
Today a 65 year old patient showed up in the office. He had not seen me for last 5 years for whatever reason and now needed a surgical clearance. He worked as a RN at a Houston Hospital and subsequently at the VA Hospital;
I did a routine EKG as follows:
It was unchanged from his previous EKGs from years ago. When he was following with me, he had a cardiac workup including imaging tests showing normal coronaries.
On taking his interval history, I found some interesting facts. While working at the VA he had some atypical chest pain. He went to the ER and had an EKG and was seen by a cardiologist stat. He was rushed to the catheterization lab and had a diagnostic cardiac catheterization which showed normal coronaries. A few months later he had similar chest pain and again went to the ER at a premier hospital in town for evaluation. An EKG was done and STEMI was called immediately. He protested to the cardiologist that he had cardiac catheterization a few months ago and that it was normal! The cardiologist was insistent that he have another one since his EKG showed that he was having a heart attack and could die. His protests were to no avail and he was rushed to the lab and had another diagnostic cardiac study which of course showed normal coronaries. The cardiologist came and apologised to him for not listening to him.
Now it was my turn to beat him on the head and tell him: ” You have STEMI written on your forehead. Wherever, you go you will be treated with emergency response and the STEMI will be summoned and you will be rushed in an elevator with a security guard holding it! Once in the cath lab you will be surrounded by a frantic team counting minutes!
So this is what you are going to do. You will take a copy of your EKG, go to Office Depot and have it reduced and laminated; then carry it with you in your wallet and if you land in the ER and before they wheel you away to the cath lab, show them the EKG and tell them that your EKG is always abnormal and that they should compare to see if there are any changes. Otherwise you will someday end up with a clot in your hand or leg or some other complication!
I think he got the message.
No offence meant and take it in the lighter vein, but I am sure every interventional cardiologist taking emergency calls faces these alarms and the 90 minutes door to balloon time does not allow much margin to hunt for old EKGs!
Case of the Week – A Foot In The Door May Be All You Need!
Here is a complicated RCA intervention from this week with several discussion points. There is a bonus here – my technique for changing guides over a coronary wire. There are several sequences – but not as many as there could have been!
Baseline angio. 73 year old woman with severe angina – history of bypass with failed RCA graft. Has critical ISR at the RCA ostium. The referring had difficulty stabilizing a JR4 guide and was unable to wire the stenosis.
Here the initial wiring sequence. We used an AL1 to engage the ostium as best as we could. We used a Fielder XT to wire the ISR – it is the perfect wire to do this because of the tapered tip, the polymer jacket and the supportive shaft.
But that AL1 position is not ideal for working. The next is to build up support. We used a TurnPike LP to dilate the channel and switch out for an exchange length wiggle wire. TP LP is ideal because of its double nitinol braid – it can drive itself forward even when support is suboptimal. Once the wire is in, we can dilate with a long balloon. IVUS to follow.
Here is the initial IVUS. The entire RCA is diseased. There is likely geographic miss distally and an underexpanded stent, but they landed it perfectly at the ostium. An AL1 is not the best guide for the remaining sequence which involves engaging and disengaging the RCA ostium. So we decided to switch guides.
Here the entire sequence to switch the guides over a coronary wire. You need a long (preferably supportive) coronary wire, and exchange length 0.035 wire, and patience!!! The 0.035 wire straightens out the AL1 during transfer.
Here is the post IVL result by IVUS. The calcium ring is disrupted is several places!
After using a 4 mm NC balloon, we implanted a 4 x 48 mm SYNERGY. Here is the post stent IVUS. We post dilated with a 4 mm NC balloon.
Here is the final result! You can see the contrast in size between the stented segment and the native, diseased RCA. There is always a risk of ‘over stretching’ the vessel when IVUS measurements are strictly followed, but this is an acceptable ’step down’.
QUESTIONS: AA Salman bhai, I had 3 questions for my own learning, not questioning. Angiographically its a beautiful result as expected from you.
is the stent truly undersized or just underexpanded (heavy calcium) in some areas by the original operator?
any for shockwave or laser (not great for calcium ) to help expand the calcium. on your post ivus the calcium appears to prevent expansion but angiographically looks awesome. risk (calcium perf ) /reward of expanding this area with a short 4.25 NC given his prior restenosis and ostial location. i would have left it as you did,
why wiggle wire? what other wire if not wiggle wire?
Good questions.
1) Undersized versus under expanded? Difficult to say. As you know, most stents between 2.5 and 3.5 mm are the same size. The difference is in the size of the balloon that they are mounted on. (@Waqas T. Qureshi MD Bhai can confirm or refute this). So, it is difficult to say whether the stent was just undersized from the get-go or not fully expanded. But it is clear that there is geographic miss and under preparation of the vessel.
2) Absolutely. I highly recommend aggressive post dilation after any atherectomy or IVL. You have to ensure the vessel will expand before the deploying another stent.
2b) This also highlights the limitation of angiography alone to gauge vessel size in diffusely diseased arteries.
2c) Post dilation options include noncompliant balloons and (now) OPN.
3) Any supportive wire may have worked. I like to use the wiggle when dealing with torturous RCAs or LADs. The wiggle portion often locks the wire in position, adding to the support provided by the wire. Of course, any other support wire may have also worked.